2
2
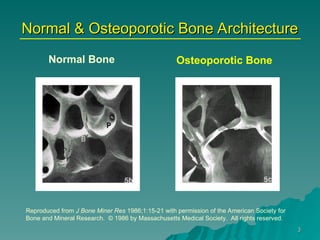
What is Osteoporosis?
Whatis Osteoporosis?
A condition in which the infrastructure
A condition in which the infrastructure
of bone becomes thin and weakened.
of bone becomes thin and weakened.
Weakened bone is at higher risk for
Weakened bone is at higher risk for
fracture to occur from minimal
fracture to occur from minimal
stresses.
stresses.
4
4
Who Gets Osteoporosis?
WhoGets Osteoporosis?
ANYONE could be at risk for Osteoporosis
ANYONE could be at risk for Osteoporosis
Most people are identified after age 50
Most people are identified after age 50
Some diseases & conditions increase risk
Some diseases & conditions increase risk
Even men & children are at risk
Even men & children are at risk
5.
5
5
Risk Factors You
RiskFactors You Can’t
Can’t Change
Change
•
Age
Age
•
Gender (4/5 cases are female)
Gender (4/5 cases are female)
•
Postmenopausal status
Postmenopausal status
•Family history, race (Caucasian or Asian),
Family history, race (Caucasian or Asian),
Vit D genetics
Vit D genetics
•Small frame (<127 lb = osteoporosis risk)
Small frame (<127 lb = osteoporosis risk)
•
Hyperparathyroidism, RSD, cancer, organ
Hyperparathyroidism, RSD, cancer, organ
replacement
replacement
•Necessary medications (steroids,
Necessary medications (steroids,
antiseizure, anticoagulants, synthroid, many
antiseizure, anticoagulants, synthroid, many
chemotherapies, some diuretics)
chemotherapies, some diuretics)
(National Osteoporosis Foundation, 2002)
6.
6
6
Additional Risk Factors
AdditionalRisk Factors
Diseases that Are Often Treated with
Glucocorticoid Medications*
Asthma
Asthma
Bursitis
Bursitis
Crohn’s Disease
Crohn’s Disease
Chronic Active
Chronic Active
Hepatitis
Hepatitis
Dermatitis (Severe)
Dermatitis (Severe)
Glaucoma
Glaucoma
Lupus Erythematosus
Lupus Erythematosus
Multiple Sclerosis
Multiple Sclerosis
Osteoarthritis
Osteoarthritis
Psoriasis
Psoriasis
Rheumatoid Arthritis
Rheumatoid Arthritis
*Partial List (National Osteoporosis Foundation, 2002)
7.
7
7
Risk Factors You
RiskFactors You Can
Can Change
Change
• Diet – inadequate calcium and vitamin D,
Diet – inadequate calcium and vitamin D,
too much or too little protein
too much or too little protein
• Some bone-damaging medications
Some bone-damaging medications
• Unhealthy lifestyle choices
Unhealthy lifestyle choices
• Alcohol (more than 2 drinks/day)
Alcohol (more than 2 drinks/day)
• Smoking (any!)
Smoking (any!)
• Too little exercise
Too little exercise
• Under-eating (<127 lb = osteoporosis risk)
Under-eating (<127 lb = osteoporosis risk)
(National Osteoporosis Foundation, 2002)
8.
8
8
Age in Years
1020 30 40 50 60 70 80 90
Active
Growth
Slow
Loss
Rapid
Loss
Less Rapid
Loss
Bones build mass beginning at birth and peak by
Bones build mass beginning at birth and peak by
age 20-30
age 20-30
Peak bone mass is attained between 25 & 30 y/o
• 50% accrued during teen years
• Declines by 1 – 1.5%/ year after peak
• Declines by 3 – 5%/ year 1st
5 yr/ menopause
Bone Development
(National
Osteoporosis
Foundation, 2002)
9.
9
9
Calcium and Bone
Recommended daily calcium intake
Recommended daily calcium intake
• Children and Young Adults
Children and Young Adults
• 1-10 years
1-10 years 800 mgs
800 mgs
• 11-24 years
11-24 years 1,200 mgs
1,200 mgs
• Adults
Adults 1,000 mgs
1,000 mgs
• Pregnant and Lactating Women
Pregnant and Lactating Women 1,200 mgs
1,200 mgs
• Postmenopausal Women Not on ERT 1,500 mgs
Postmenopausal Women Not on ERT 1,500 mgs
• Men over the age of 65
Men over the age of 65 1,500 mgs
1,500 mgs
(National Osteoporosis Foundation, 2002)
Excess
Excess salt displaces calcium
salt displaces calcium
– Is added to almost all
Is added to almost all canned foods
canned foods!
!
High
High phosphates leach calcium
phosphates leach calcium from bone!
from bone!
– Soda
Soda – the worst culprit
– the worst culprit
10.
10
10
Bone Nutrition -Beyond Calcium
Vitamin D
Vitamin D
• At least 800 units daily
At least 800 units daily (Boonen S et al, 2006; Pfeifer M et al, 2002)
)
• 30 minutes of sun to hands & face daily sufficient in sub-tropical
30 minutes of sun to hands & face daily sufficient in sub-tropical
latitudes but only the “sunny” 6 months in temperate latitudes
latitudes but only the “sunny” 6 months in temperate latitudes
Magnesium
Magnesium
• 400-600/day
400-600/day – allows calcification as a natural calcium
– allows calcification as a natural calcium
chelator
chelator (Barzel US, 1998)
• Depleted by stress, physical exertion
Depleted by stress, physical exertion
Protein Intake and Bone - moderation is the key
oderation is the key
• Women (35-59 y/o) w/ protein intake >95g/day (5 servings red
Women (35-59 y/o) w/ protein intake >95g/day (5 servings red
meat/wk) vs those <59 g/day had increased risk of forearm fractures
meat/wk) vs those <59 g/day had increased risk of forearm fractures
(Feskanich D et al, 1996)
• High amounts of protein intake (~200 g/day) associated with
High amounts of protein intake (~200 g/day) associated with
decreased bone density
decreased bone density (Barzel US 1998)
• Low protein diets (<50g/day) associated with decreased bone density
Low protein diets (<50g/day) associated with decreased bone density
(Chiu JF et al 1997)
11.
11
11
Drug Options –FDA approved
Anti-resorptives (slow bone resorption)
Anti-resorptives (slow bone resorption)
• Bisphosphonates (alendronate, risedronate,
Bisphosphonates (alendronate, risedronate,
ibandronate, pamidronate)
ibandronate, pamidronate) (Wasnich RD et al, 2004;
(Wasnich RD et al, 2004;
Chestnut III CH et al, 2004, Chan SS et al, 2004)
Chestnut III CH et al, 2004, Chan SS et al, 2004)
• Selective estrogen receptor modulators
Selective estrogen receptor modulators
(raloxifene)
(raloxifene)
• Calcitonin (Miacalcin)
Calcitonin (Miacalcin)
• Estrogen
Estrogen (Writing Group WHI, 2002; Nerhood RC 2001)
(Writing Group WHI, 2002; Nerhood RC 2001)
• Risks with long-term use may outweigh benefits,
Risks with long-term use may outweigh benefits,
may be safer with lower doses
may be safer with lower doses
• Always needs to be given with progesterone when
Always needs to be given with progesterone when
uterus present
uterus present
Anabolic (bone forming)
Anabolic (bone forming)
• Parathyroid hormone (teraparatide)
Parathyroid hormone (teraparatide) (Heaney RP,
(Heaney RP,
2003)
2003)
12.
12
12
Why Do BonesWeaken?
Why Do Bones Weaken?
Bones depend on calcium, other
Bones depend on calcium, other
chemicals, and vitamins to keep them
chemicals, and vitamins to keep them
strong.
strong.
Bones grow as a response to physical
Bones grow as a response to physical
stress being put on them.
stress being put on them.
The density (hardness) of bones
The density (hardness) of bones
requires a good diet, some sunlight,
requires a good diet, some sunlight,
and exercise in order to stay strong
and exercise in order to stay strong
and not break.
and not break.
13.
13
13
It’s a BigProblem
It’s a Big Problem
Osteoporosis affects more than 10
Osteoporosis affects more than 10
million people in the US
million people in the US
8 million women
8 million women
2 million men (but they are catching up)
2 million men (but they are catching up)
24 million others have low bone
24 million others have low bone
mass, called osteopenia
mass, called osteopenia
Osteopenia is a precursor to
Osteopenia is a precursor to
osteoporosis
osteoporosis
(National Osteoporosis Foundation, 2002)
14.
14
14
Why is Ita Problem?
Why is It a Problem?
Osteoporosis, by itself, is not a
Osteoporosis, by itself, is not a
problem. It doesn’t cause pain and
problem. It doesn’t cause pain and
you will not know you have it
you will not know you have it!
!
The problem is that it makes bones
The problem is that it makes bones
very brittle and brittle bones can
very brittle and brittle bones can
break easily.
break easily.
A broken bone is called a FRACTURE.
A broken bone is called a FRACTURE.
15.
15
15
Fracture Numbers
Fracture Numbers
Every year there are 1.5 million bone fractures in
Every year there are 1.5 million bone fractures in
this country
this country
300,000 hip fractures
300,000 hip fractures
700,000 vertebral fractures
700,000 vertebral fractures
250,000 wrist fractures
250,000 wrist fractures
Women have a greater lifetime risk of sustaining
Women have a greater lifetime risk of sustaining
a hip fracture than breast, ovarian , and uterine
a hip fracture than breast, ovarian , and uterine
cancer combined
cancer combined
Fracture care costs
Fracture care costs $3 BILLION
$3 BILLION every year!
every year!
(National Osteoporosis Foundation, 2002)
16.
16
16
Fractures HURT
Fractures HURT
Fracturescause:
Fractures cause:
Pain
Pain
Limited mobility
Limited mobility
• Prolonged bedrest causes:
Prolonged bedrest causes:
Loss of strength
Loss of strength
Pneumonia
Pneumonia
Disability
Disability
Death
Death
• 20% of those with hip fractures die within one year
20% of those with hip fractures die within one year
• Increased mortality with each vertebral fracture
Increased mortality with each vertebral fracture
(National Osteoporosis Foundation, 2002)
17.
17
17
Determinants
Determinants of
of
Osteoporotic Fracture
OsteoporoticFracture
Number of
Number of
osteoporosis
osteoporosis
risk factors
risk factors
Forward
Forward
bending
bending
(trunk flexion)
(trunk flexion)
Poor balance,
Poor balance,
or accidents
or accidents
resulting in
resulting in
falls
falls
Vertebral Fracture Hip Fracture
18.
18
18
Fracture Force RisksDuring
Bending and Lifting
Compression loads imposed on
Compression loads imposed on
the L3 motion segment (lower
the L3 motion segment (lower
back) by
back) by 30º of trunk flexion
30º of trunk flexion
– 1800 N with
1800 N with arms at chest
arms at chest
– 2610 N with arms in front,
2610 N with arms in front, holding 2
holding 2
kg in each hand
kg in each hand (Schultz et al 1982
(Schultz et al 1982)
)
300 to 1200 N enough to fracture
300 to 1200 N enough to fracture
an osteoporotic vertebra
an osteoporotic vertebra (Edmondston et
(Edmondston et
al 1997)
al 1997)
Practical Application -
Practical Application - bend and
lift in everyday life with the trunk
in relative neutral!
19.
19
19
Exercise and VertebralFractures
Exercise and Vertebral Fractures
(for women with a previous fracture)
(for women with a previous fracture)
Type of Exercise
Type of Exercise
Spinal Extension (Back
Spinal Extension (Back
arches/lifts)
arches/lifts)
Spinal Flexion
Spinal Flexion
(Crunches)
(Crunches)
Combined Flexion and
Combined Flexion and
Extension
Extension
No exercise
No exercise
New Fractures
New Fractures
16%
16%
89%
89%
53%
53%
67%
67%
(Sinaki and Mikkelson, 1984)
(Sinaki and Mikkelson, 1984)
20.
20
20
How Do IKnow if I Have It?
How Do I Know if I Have It?
There are many types of screening tests
There are many types of screening tests
available in the community. Many use a
available in the community. Many use a
finger or a foot to estimate possible risk.
finger or a foot to estimate possible risk.
The gold standard (the absolute test) for
The gold standard (the absolute test) for
determining the amount of bone density
determining the amount of bone density
an individual has is a
an individual has is a DEXA test
DEXA test. It is like
. It is like
an X-ray without the radiation.
an X-ray without the radiation.
You lie on a table and a scanner passes
You lie on a table and a scanner passes
over you. A computer determines how
over you. A computer determines how
much bone you have by the information
much bone you have by the information
read by the scanner.
read by the scanner.
21.
21
21
What’s a T-score?
What’sa T-score?
The amount of bone you have is
The amount of bone you have is
determined by how much has been lost
determined by how much has been lost
since childhood, assuming you had lots of
since childhood, assuming you had lots of
calcium and activity at that time
calcium and activity at that time
A T-score is a statistical number which
A T-score is a statistical number which
says whether you are above or below
says whether you are above or below
“normal”
“normal”
T-scores are such numbers as -1.4 or -3.0
T-scores are such numbers as -1.4 or -3.0
or even + 1.0 sometimes.
or even + 1.0 sometimes.
22.
22
22
T-scores
T-scores
Normal T-scoresrange from +1 to -1
Normal T-scores range from +1 to -1
Osteopenia
Osteopenia T-scores
T-scores
-1.0 to -2.5
-1.0 to -2.5
Osteoporosis
Osteoporosis T-score
T-score
less than -2.5
less than -2.5 (up to -6.0)
(up to -6.0)
23.
23
23
What Should IDo First?
What Should I Do First?
There are 3 major things you can do
There are 3 major things you can do
1.
1. Talk to your
Talk to your doctor
doctor about a Bone Density
about a Bone Density
Test
Test
2.
2. Talk to a
Talk to a physical therapist
physical therapist about your
about your
activity level and an exercise program to
activity level and an exercise program to
combat osteoporosis
combat osteoporosis
3.
3. Talk to a
Talk to a dietician
dietician to make sure your diet
to make sure your diet
is providing your bones with enough
is providing your bones with enough
calcium and is balanced correctly
calcium and is balanced correctly
24.
24
24
What If IAlready Have Osteoporosis?
What If I Already Have Osteoporosis?
Talk to your physician and pharmacist
Talk to your physician and pharmacist
about
about medications
medications available to help you
available to help you
Make sure your
Make sure your diet
diet includes enough
includes enough
calcium, not too much caffeine or alcohol,
calcium, not too much caffeine or alcohol,
and adequate, but not excessive, protein.
and adequate, but not excessive, protein.
Spend at least 30 minutes/day in sunlight
Spend at least 30 minutes/day in sunlight
and/or eat foods which are fortified with
and/or eat foods which are fortified with
Vitamin D
Vitamin D
and………………..
and………………..
25.
25
25
See a PhysicalTherapist
See a Physical Therapist
PTs are able to develop an exercise
PTs are able to develop an exercise
program for you that will be appropriate
program for you that will be appropriate
for your condition
for your condition
PTs will evaluate your posture, your
PTs will evaluate your posture, your
strength, your range of motion, your
strength, your range of motion, your
balance, and your general endurance
balance, and your general endurance
status
status
PTs will develop a balanced program which
PTs will develop a balanced program which
should help keep you fit as well as safe
should help keep you fit as well as safe
PTs can answer your questions or refer
PTs can answer your questions or refer
you to others who will
you to others who will
26.
26
26
Studies on Exercise
Studieson Exercise
Appropriate exercise may slow the
Appropriate exercise may slow the
rate of bone loss
rate of bone loss
Sedentary lifestyles and immobility
Sedentary lifestyles and immobility
lower bone density
lower bone density
Effects of exercise are improved
Effects of exercise are improved
when combined with proper nutrition
when combined with proper nutrition
and medication
and medication
27.
27
27
Exercise Effect onBone –
Exercise Effect on Bone –
Works only when “Regular”
Works only when “Regular”
Postmenopausal women exercised
Postmenopausal women exercised
3 times per week for 9 months
3 times per week for 9 months
Stair-climbing for ~ 30 minutes
Stair-climbing for ~ 30 minutes
each session
each session
Spinal bone density
Spinal bone density
4% in
4% in
exercisers
exercisers
Spinal bone density
Spinal bone density
to baseline
to baseline
within 9 months for those who
within 9 months for those who
stopped exercising
stopped exercising
(Dalsky 1988)
28.
28
28
Resistance Training
Increases BoneDensity Best
Landmark study (
Landmark study (Nelson & Fiaterone 1994)
Nelson & Fiaterone 1994)
– Sedentary 50-70 y/o postmenopausal women
Sedentary 50-70 y/o postmenopausal women
– Resistance training 2 X/wk on 5 machines for 1
Resistance training 2 X/wk on 5 machines for 1
year
year
– Significant bone density increases in spine, hip,
Significant bone density increases in spine, hip,
total body
total body
Many other studies validate, including:
Many other studies validate, including:
– Cussler EC 2003
Cussler EC 2003
– Kerr D 2001
Kerr D 2001
– Kelley GA 2001
Kelley GA 2001
29.
29
29
Principles of Exercisefor
Principles of Exercise for
People with Lowered Bone Mass
People with Lowered Bone Mass
Posture
Posture is critical in all activities
is critical in all activities
Weight bearing
Weight bearing is important
is important
Walking, Dancing, Stair climbing
Walking, Dancing, Stair climbing
Resistance exercise
Resistance exercise is the best way
is the best way
to strengthen bone & muscle groups
to strengthen bone & muscle groups
Balance exercise
Balance exercise to decrease fall risk
to decrease fall risk
Avoid activities or positions that
Avoid activities or positions that
move the body into bent (flexed)
move the body into bent (flexed)
postures
postures
30.
30
30
Exercise Intervention Works
ExerciseIntervention Works
After Vertebral fracture
After Vertebral fracture
– 6 months of supervised exercise
6 months of supervised exercise
back strength
back strength
and psychological status
and psychological status (Gold et al:
(Gold et al: 2004)
2004)
For kyphosis and balance
For kyphosis and balance
– 12 weeks of SAFE yoga (
12 weeks of SAFE yoga (no forward bending!!!
no forward bending!!!)
)
improves balance & posture
improves balance & posture (Greendale et al, 2002)
(Greendale et al, 2002)
For osteoporosis and back pain
For osteoporosis and back pain
– 10 weeks of combination group and
10 weeks of combination group and
individual exercise increases height,
individual exercise increases height,
improves back posture and strength
improves back posture and strength (Lindsey
(Lindsey
et al, 1995)
et al, 1995)
31.
31
31
Eclectic Treatment FocusEssential
Eclectic Treatment Focus Essential
Frailty Injury Cooperative Interventions
Frailty Injury Cooperative Interventions
Trial Analysis revealed that a year after
Trial Analysis revealed that a year after
the intervention:
the intervention:
– Fall rate decreased
Fall rate decreased 10%
10% in those who did
in those who did
strength
strength exercises only
exercises only
– Fall rate decreased by
Fall rate decreased by 17%
17% in those who
in those who
received
received “balance” exercises
“balance” exercises only
only
– Fall rate decreased by
Fall rate decreased by 31%
31% in those who did
in those who did
both plus the Tai Chi.
both plus the Tai Chi.
(Wolfson L et al: Balance and strength training in older adults:
(Wolfson L et al: Balance and strength training in older adults:
intervention gains and Tai Chi maintenance. 1996)
intervention gains and Tai Chi maintenance. 1996)
– Those who increase
Those who increase all balance scores
all balance scores
show a
show a 60%
60% reduction in fall risk.
reduction in fall risk.
(Tinetti ME et al: A multifactorial intervention to reduce the risk of
(Tinetti ME et al: A multifactorial intervention to reduce the risk of
falling among elderly people living in the community. 1994)
falling among elderly people living in the community. 1994)
See a PhysicalTherapist
See a Physical Therapist
for More Details!
for More Details!
http://www.apta.org
http://www.apta.org
Click the “Find a PT” button
Click the “Find a PT” button
34.
34
34
Find Out MoreAbout Osteoporosis
Find Out More About Osteoporosis
Web sites for up to date information:
Web sites for up to date information:
www.geriatricspt.org/clients/resources.cfm
www.geriatricspt.org/clients/resources.cfm
www.nof.org
www.nof.org
www.surgeongeneral/library/bonehealth
www.surgeongeneral/library/bonehealth
www.osteo.org
www.osteo.org
www.fore.org
www.fore.org
35.
35
35
References
References
1.
1. Barzel US,Massey LK. Excess dietary protein can adversely affect bone.
Barzel US, Massey LK. Excess dietary protein can adversely affect bone. J
J
Nutr.
Nutr. Jun 1998;128(6):1051-1053.
Jun 1998;128(6):1051-1053.
2.
2. Boonen S, Vanderschueren D, Haentjens P, Lips P. Calcium and vitamin D
Boonen S, Vanderschueren D, Haentjens P, Lips P. Calcium and vitamin D
in the prevention and treatment of osteoporosis - a clinical update.
in the prevention and treatment of osteoporosis - a clinical update. J Intern
J Intern
Med.
Med. Jun 2006;259(6):539-552.
Jun 2006;259(6):539-552.
3.
3. Chan SS, Nery LM, McElduff A, et al. Intravenous pamidronate in the
Chan SS, Nery LM, McElduff A, et al. Intravenous pamidronate in the
treatment and prevention of osteoporosis.
treatment and prevention of osteoporosis. Intern Med J.
Intern Med J. Apr
Apr
2004;34(4):162-166.
2004;34(4):162-166.
4.
4. Chesnut III CH, Skag A, Christiansen C, et al. Effects of oral ibandronate
Chesnut III CH, Skag A, Christiansen C, et al. Effects of oral ibandronate
administered daily or intermittently on fracture risk in postmenopausal
administered daily or intermittently on fracture risk in postmenopausal
osteoporosis.
osteoporosis. J Bone Miner Res.
J Bone Miner Res. Aug 2004;19(8):1241-1249.
Aug 2004;19(8):1241-1249.
5.
5. Chiu JF, Lan SJ, Yang CY, et al. Long-term vegetarian diet and bone
Chiu JF, Lan SJ, Yang CY, et al. Long-term vegetarian diet and bone
mineral density in postmenopausal Taiwanese women.
mineral density in postmenopausal Taiwanese women. Calcif Tissue Int.
Calcif Tissue Int.
Mar 1997;60(3):245-249.
Mar 1997;60(3):245-249.
6.
6. Cussler EC, Lohman TG, Going SB, et al. Weight lifted in strength training
Cussler EC, Lohman TG, Going SB, et al. Weight lifted in strength training
predicts bone change in postmenopausal women.
predicts bone change in postmenopausal women. Med Sci Sports Exerc.
Med Sci Sports Exerc.
Jan 2003;35(1):10-17.
Jan 2003;35(1):10-17.
7.
7. Dalsky GP, Stocke KS, Ehsani AA, Slatopolsky E, Lee WC, Birge SJ Jr.
Dalsky GP, Stocke KS, Ehsani AA, Slatopolsky E, Lee WC, Birge SJ Jr.
Weight-bearing exercise training and lumbar bone mineral content in
Weight-bearing exercise training and lumbar bone mineral content in
postmenopausal women.
postmenopausal women. Ann Intern Med.
Ann Intern Med. Jun 1988;108(6):824-828.
Jun 1988;108(6):824-828.
8.
8. Edmondston SJ, Singer KP, Day RE, Price RI, Breidahl PD. Ex vivo
Edmondston SJ, Singer KP, Day RE, Price RI, Breidahl PD. Ex vivo
estimation of thoracolumbar vertebral body compressive strength: the
estimation of thoracolumbar vertebral body compressive strength: the
relative contributions of bone densitometry and vertebral morphometry.
relative contributions of bone densitometry and vertebral morphometry.
Osteoporos Int.
Osteoporos Int. 1997;7(2):142-148.
1997;7(2):142-148.
9.
9. Feskanich D, Willett WC, Stampfer MJ, Colditz GA. Protein consumption and
Feskanich D, Willett WC, Stampfer MJ, Colditz GA. Protein consumption and
bone fractures in women.
bone fractures in women. Am J Epidemiol.
Am J Epidemiol. Mar 1 1996;143(5):472-479.
Mar 1 1996;143(5):472-479.
36.
36
36
References (Cont)
References (Cont)
10.GoldDT, Shipp KM, Pieper CF, Duncan PW, Martinez S, Lyles KW. Group
10.Gold DT, Shipp KM, Pieper CF, Duncan PW, Martinez S, Lyles KW. Group
treatment improves trunk strength and psychological status in older
treatment improves trunk strength and psychological status in older
women with vertebral fractures: results of a randomized, clinical trial.
women with vertebral fractures: results of a randomized, clinical trial. J Am
J Am
Geriatr Soc.
Geriatr Soc. Sep 2004;52(9):1471-1478.
Sep 2004;52(9):1471-1478.
11.Greendale GA, McDivit A, Carpenter A, Seeger L, Huang MH. Yoga for
11.Greendale GA, McDivit A, Carpenter A, Seeger L, Huang MH. Yoga for
women with hyperkyphosis: results of a pilot study.
women with hyperkyphosis: results of a pilot study. Am J Public Health.
Am J Public Health.
Oct 2002;92(10):1611-1614.
Oct 2002;92(10):1611-1614.
12.Heaney RP. Advances in therapy for osteoporosis.
12.Heaney RP. Advances in therapy for osteoporosis. Clin Med Res.
Clin Med Res. Apr
Apr
2003;1(2):93-99.
2003;1(2):93-99.
13.Herbold NH, Frates SE. Update of nutrition guidelines for the teen: trends
13.Herbold NH, Frates SE. Update of nutrition guidelines for the teen: trends
and concerns.
and concerns. Curr Opin Pediatr.
Curr Opin Pediatr. Aug 2000;12(4):303-309.
Aug 2000;12(4):303-309.
14.Kelley GA, Kelley KS, Tran ZV. Resistance training and bone mineral
14.Kelley GA, Kelley KS, Tran ZV. Resistance training and bone mineral
density in women: a meta-analysis of controlled trials.
density in women: a meta-analysis of controlled trials. Am J Phys Med
Am J Phys Med
Rehabil.
Rehabil. Jan 2001;80(1):65-77.
Jan 2001;80(1):65-77.
15.Kelley GA, Kelley KS, Tran ZV. Exercise and lumbar spine bone mineral
15.Kelley GA, Kelley KS, Tran ZV. Exercise and lumbar spine bone mineral
density in postmenopausal women: a meta-analysis of individual patient
density in postmenopausal women: a meta-analysis of individual patient
data.
data. J Gerontol A Biol Sci Med Sci.
J Gerontol A Biol Sci Med Sci. Sep 2002;57(9):M599-604.
Sep 2002;57(9):M599-604.
16.Kerr D, Ackland T, Maslen B, Morton A, Prince R. Resistance training over 2
16.Kerr D, Ackland T, Maslen B, Morton A, Prince R. Resistance training over 2
years increases bone mass in calcium-replete postmenopausal women.
years increases bone mass in calcium-replete postmenopausal women. J
J
Bone Miner Res.
Bone Miner Res. Jan 2001;16(1):175-181.
Jan 2001;16(1):175-181.
17.Lindsey C, Reisine S, Fertig J. Evaluation for the effects of exercise on
17.Lindsey C, Reisine S, Fertig J. Evaluation for the effects of exercise on
posture, back strength, pain & mood in postmenopausal women with
posture, back strength, pain & mood in postmenopausal women with
osteoporosis & back pain. Paper presented at: WCPT, 1995; Washington,
osteoporosis & back pain. Paper presented at: WCPT, 1995; Washington,
DC.
DC.
18.National_Osteoporosis_Foundation.
18.National_Osteoporosis_Foundation. America's Bone Health: The
America's Bone Health: The
State of Osteoporosis and Low Bone Mass in Our Nation.
State of Osteoporosis and Low Bone Mass in Our Nation.
Washington, DC: National Osteoporosis Foundation; 2002.
Washington, DC: National Osteoporosis Foundation; 2002.
37.
37
37
References (cont)
References (cont)
19.
19.NelsonME, Fiatarone MA, Morganti CM, Greenberg RA, Evans WJ. Effects of
Nelson ME, Fiatarone MA, Morganti CM, Greenberg RA, Evans WJ. Effects of
high-intensity strength training on multiple risk factors for osteoporotic
high-intensity strength training on multiple risk factors for osteoporotic
fractures: a randomized controlled trial.
fractures: a randomized controlled trial. JAMA.
JAMA. Dec 28 1994;272(24):1909-
Dec 28 1994;272(24):1909-
1914.
1914.
20.
20.Schultz AB, Andersson GBJ, Haderspeck K, et. al.
Schultz AB, Andersson GBJ, Haderspeck K, et. al. Analysis and
Analysis and
measurement of lumbar trunk loads in tasks involving bends and twists.
measurement of lumbar trunk loads in tasks involving bends and twists. J
J
Biomechanics.
Biomechanics. 1982;15(9):669-675.
1982;15(9):669-675.
21.
21.Sinaki M, Itoi E, Wahner HW, et al. Stronger back muscles reduce the
Sinaki M, Itoi E, Wahner HW, et al. Stronger back muscles reduce the
incidence of vertebral fractures: a prospective 10 year follow-up of
incidence of vertebral fractures: a prospective 10 year follow-up of
postmenopausal women.
postmenopausal women. Bone.
Bone. Jun 2002;30(6):836-841.
Jun 2002;30(6):836-841.
22.
22.Sinaki M, Mikkelsen BA. Postmenopausal spinal osteoporosis: flexion versus
Sinaki M, Mikkelsen BA. Postmenopausal spinal osteoporosis: flexion versus
extension exercises.
extension exercises. Arch Phys Med Rehabil.
Arch Phys Med Rehabil. Oct 1984;65(10):593-596.
Oct 1984;65(10):593-596.
23.
23.Tinetti ME, Baker DI, McAvay G, et al. A multifactorial intervention to reduce
Tinetti ME, Baker DI, McAvay G, et al. A multifactorial intervention to reduce
the risk of falling among elderly people living in the community.
the risk of falling among elderly people living in the community. N Engl J
N Engl J
Med.
Med. Sep 29 1994;331(13):821-827.
Sep 29 1994;331(13):821-827.
24.
24.Wasnich RD, Bagger YZ, Hosking DJ, et al.
Wasnich RD, Bagger YZ, Hosking DJ, et al. Changes in bone density and
Changes in bone density and
turnover after alendronate or estrogen withdrawal.
turnover after alendronate or estrogen withdrawal. Menopause.
Menopause. Nov-Dec
Nov-Dec
2004;11((6 Pt 1)):622-630.
2004;11((6 Pt 1)):622-630.
25.
25.Wolfson L, Whipple R, Derby C, et al. Balance and strength training in older
Wolfson L, Whipple R, Derby C, et al. Balance and strength training in older
adults: intervention gains and Tai Chi maintenance.
adults: intervention gains and Tai Chi maintenance. J Am Geriatr Soc.
J Am Geriatr Soc. May
May
1996;44(5):498-506.
1996;44(5):498-506.
26.
26.Writing Group for the Women's Health Initiative Investigators. Risks and
Writing Group for the Women's Health Initiative Investigators. Risks and
benefits of estrogen plus progestin in healthy postmenopausal women:
benefits of estrogen plus progestin in healthy postmenopausal women:
principal results From the Women's Health Initiative randomized controlled
principal results From the Women's Health Initiative randomized controlled
trial.
trial. JAMA.
JAMA. Jul 17 2002;288(3):321-333.
Jul 17 2002;288(3):321-333.
Editor's Notes
#8 Bone growth is promoted by adequate intake of calcium, vitamin D, protein and exercise