Content
Success Always BelongsFor Those
Who Are Prepared
• Introduction
• Etiology (Pathophysiology)
• Clinical features
• Classification
• Microbiology
• Management
3.
Introduction
• First describedby Hippocrates (460-730BC) as infection after fracture
• Earliest description is from William Bromfieled in 1773 describing hematogenous
osteomyelitis
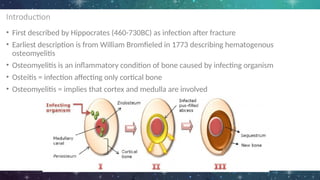
• Osteomyelitis is an inflammatory condition of bone caused by infecting organism
• Osteitis = infection affecting only cortical bone
• Osteomyelitis = implies that cortex and medulla are involved
4.
Introduction
• Before introductionof Penicillin in 1940, surgical management is mainstay of
treatment
• High rate of mortality due to sepsis
5.
Etiology/Pathophysiology
• According toLew and Waldvogel classification system
i. Hematogenous spread (20% of cases)
- most common in children
- mostly in long bones
ii. Contiguous spread (50% of cases)
- previous surgery, trauma
iii. With vascular insufficiency (30% of cases)
- poor vascularity
*not helpful in determining treatment regimen or
prognosis
6.
Pathophysiology
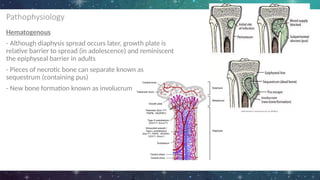
Hematogenous
• Often aftertrauma or medical intervention
• Before advent of antibiotics, hematogenous OM led to chronic infection in more than half of the
patients
• 1/4th ended up dying due to sepsis
- Usually begins at metaphysis
- It enters the nutrient artery which provide extensive network of vessels
- These vessels instead of anastomosing, they terminate in the venous sinusoids, providing ideal lake of
bacterial seeding
- Terminal branches also have low oxygen tension which inhibits action of phagocytosis
- Spreads to adjacent trabecular or cancellous bone and eventually laterally to and through cortex via
Haversian canal to the periosteum
- Periosteum may rupture. Infection in cortical bone also leads to vascular compromise which leads to
bone necrosis
7.
Pathophysiology
Hematogenous
- Although diaphysisspread occurs later, growth plate is
relative barrier to spread (in adolescence) and reminiscent
the epiphyseal barrier in adults
- Pieces of necrotic bone can separate known as
sequestrum (containing pus)
- New bone formation known as involucrum
8.
Pathophysiology
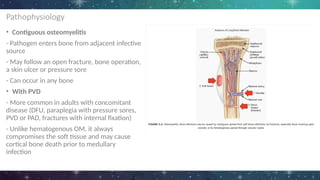
• Contiguous osteomyelitis
-Pathogen enters bone from adjacent infective
source
- May follow an open fracture, bone operation,
a skin ulcer or pressure sore
- Can occur in any bone
• With PVD
- More common in adults with concomitant
disease (DFU, paraplegia with pressure sores,
PVD or PAD, fractures with internal fixation)
- Unlike hematogenous OM, it always
compromises the soft tissue and may cause
cortical bone death prior to medullary
infection
9.
Clinical Features
• Painat involved bone
• Fever
• Unilateral localized swelling
• Erythema
• Reduced ROM
*Chronic OM (more difficult to diagnose)
- Pain (most common sx), diffuse or non specific
- signs of old healed sinuses, active discharging sinuses, soft tissue abscesses or scar from
previous surgery or injury
- chronic OM can produce long term ill health and disability
10.
Classification
● Time ofdisease onset
○ Acute (<2 weeks)
○ Subacute (2 weeks to 3 months)
○ Chronic (months to years)
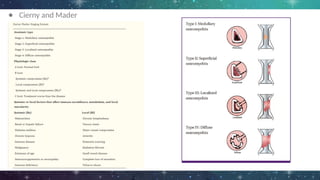
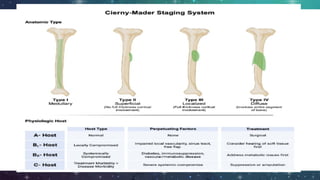
● Cierny and Mader
○ Anatomic stage
○ Host health status
Microbiology
• S. aureuscan cause all types of OM, causal
organism in over 1/3rd of acute cases and half of
all vertebral infections
• Contiguous infections arising from injury or
surgery often have poly-microbial
• In drug addicts and immuno-compromised,
atypical organisms can be cultured
• Sickle-cell disease characterized by recurrent
hypoxic crises which can produce extensive bone
infarcts that could get infected (S. aureus,
salmonella)
14.
Microbiology
• Hematogenous Mycobacteriumtuberculosis
infection of bone accounts for 1 in 50 of all cases
• Half affecting vertebral bodies, mainly in thoracic
• Required bone biopsy for confirmation of
diagnosis
• Most cases can be treated with multi-drug
antibiotic regimen and surgery reserved for those
with neurological complications or to provide
stability to spine
Imaging
● Plain filmradiography
○ Extend at least 1cm/ compromise 30 -
50% of bone mineral
○ Bone destruction may not appear until
approximately 2 weeks after onset
○ Osteolysis, periosteal reaction and
sequestra
○ Brodie’s abscess
CT scan
● Superiorthan both MRI and plain radiography in depicting bony
margins
● Identifying sequestrum and involucrum
● Sensitivity and specificity is low (67% and 50% respectively)
● Limitations:
○ Does not exclude early osteomyelitis
○ Artifact when metallic implants are present
23.
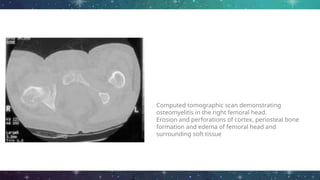
Computed tomographic scandemonstrating
osteomyelitis in the right femoral head.
Erosion and perforations of cortex, periosteal bone
formation and edema of femoral head and
surrounding soft tissue
24.
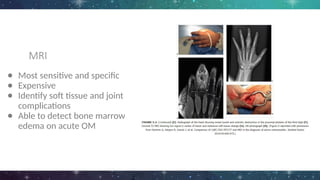
MRI
● Most sensitiveand specific
● Expensive
● Identify soft tissue and joint
complications
● Able to detect bone marrow
edema on acute OM
25.
Ultrasound
● Little rolein direct assessment of osteomyelitis
● Fast and inexpensive examination of soft tissues
● Guide drainage of soft tissue collections
● Visualise abscess, cellulitis, sub periosteal collections and joint
effusions
27.
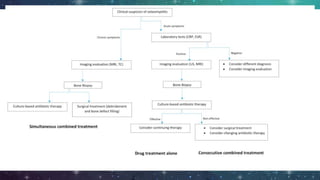
Treatment
● General considerationsin identifications of aetiology, disease classification
and understanding of pathogenesis of condition
● There are no single abx regimen or surgical procedure which is appropriate
for all patients
28.
Antibiotic therapy
● Acutehematogenous osteomyelitis
● 4 - 6 weeks course of appropriate antibiotic therapy
● Only appropriate to treat acute bone infection solely with abx in
following circumstances:
i. Dx confirmed within few days of onset of symptoms
ii. No dead bone or abscess seen on imaging
iii. Rapid systemic response to drug treatment
iv. No adjacent septic arthritis
v. Tuberculous OM
vi. Vertebral OM without cord compression
29.
Antibiotic therapy
● Treatmentshould be modified after obtaining cultures
● If there is no rapid clinical response, limb deteriorates, or imaging
evidence of progression of disease, surgery is indicated
32.
Chronic Osteomyelitis
● Characterizedby presence of dead bone colonized by bacteria
● Preventing eradication by abx alone
● Definitive treatment must include surgery
● However mx must include evaluation of:
1. Effects of disease
2. Benefits of treatment and associated risks
• Full cure of chronic osteomyelitis may involve complex
surgery with complications, antimicrobial drug reactions, staged
reconstruction and prolonged time in treatment and rehabilitation.
• An approach which arrests current symptoms, but with the potential for later
recurrence, may be more acceptable for some patients
34.
Surgical management
● Chronicosteomyelitis
● Generally managed with antibiotics and surgical debridement
● Excision of dead bone
● Reconstruction of bone segment
● Stabilization of bone
● Dead space management
Most cases ofchildhood AHOM can be treated for 20 days, including a short period intravenously, with large doses of a
well-absorbed antimicrobial such as clindamycin or a first-generation cephalosporin, provided the clinical response is good
and C-reactive protein normalizes within 7 to 10 days. Extensive surgery is rarely needed.
38.
Intravenous to oraltherapy, after 3-4 days in patients responding well, followed by oral therapy to a total of
3 weeks may be as effective as longer courses for uncomplicated acute osteomyelitis
39.
Surgery combined withanti-infective chemotherapy leads to long-lasting containment of
infection in 70% to 90% of cases. Suitable drugs are not yet available for the eradication of
biofilm-producing bacteria.
40.
Referrences
● Osteomyelitis, MartinMcNally, Kugan Nagarajah
● Osteomyelitis and Septic Arthritis, Basic Medical Key
● https://radiopaedia.org/articles/osteomyelitis
#20 Piece of devitalised bone that are separated from its surrounding bone during process of necrosis
Reservoir for infection as it is avascular and it is not penetrated by antibiotics
Encased in a thick sheath of periosteal new bone - involucrum
cloaca is an opening in an involucrum which allows drainage of purulent and necrotic material out of the dead bone. If the tract extends to the skin surface, the portion extending beyond the involucrum to the skin surface is called a sinus tract
#34 local myoplasty,
free-tissue transfers and the use of antibioticimpregnated
beads