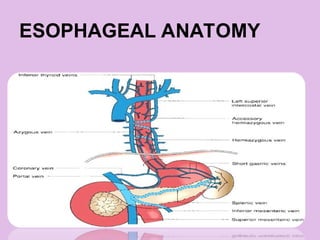
Introduction
• Esophageal perforationis rare but life
threatening emergency.
• Most lethal alimentary tract perforation.
• INCIDENCE IS TOO LOW
• MORTALITY IS TOO HIGH
Definition
• Esophageal perforation(rupture)is a tear or
hole in the esophageal wall.
• It is usually an acute injury, but slow
progessing conditions can also cause it.
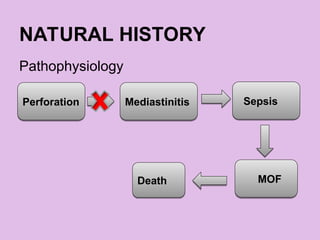
• If a rupture occurs no matter how small it is
an emergency. This is because contents
from the esophagus can escape through the
hole into the chest and bloodstream,
causing life threatening complications.
11.
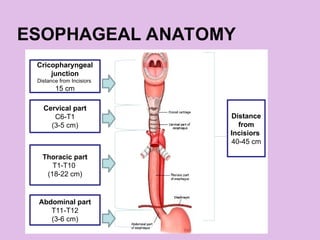
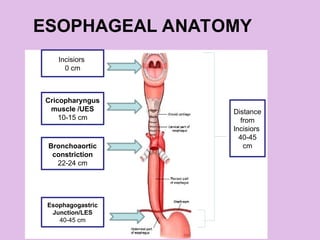
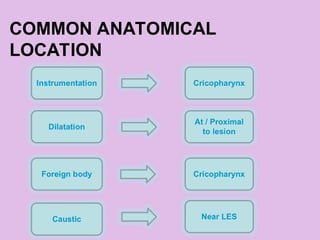
ETIOLOGY
• Increased intraluminalpressure at the
anatomical sites of narrowing, as well as
sites narrowed by a malignancy, foreign
body, or physiologic dysfunction.
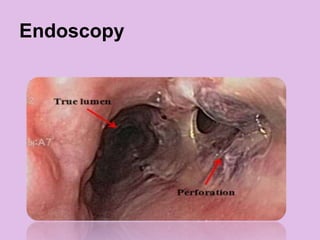
• More than one half of all esophageal
perforations are iatrogenic and most of
these occur during endoscopy.
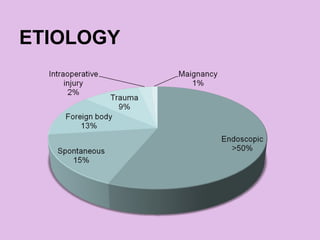
ETIOLOGY
• The estimatedrisk of esophageal perforation by
endoscopic procedure :-
Diagnostic endoscopy with a flexible endoscope 0.03 %
Diagnostic endoscopy with a rigid endoscope 0.11 %
Stricture dilation 0.09 – 2.2 %
Sclerotherapy 1-5 %
Pneumatic dilation for achalasia 2 – 6 %
14.
RISK FACTORS
• Chronicacid reflux (GERD)
• Severe esophagitis
• Prior radiation therapy
• History of caustic ingestion
• Chronic alcohol use
• Esophageal cancer
• Previous medical procedures on esophagus
• Pill Esophagitis
NSAID
KCl
ALENDRONATE (Bisphosphonates) : Px should remain upright
for >30min after ingestion
DOXYCYCLIN
15.
RISK FACTORS
• Eosinophilicesophagitis
• Complex (tortuous) or long strictures
• Presence of esophageal diverticula
• Inexperienced operator
• Use of high inflation pressures with balloon dilation
Hernandez LV, Jacobson JW, Harris MS, Hernandez LJ. Comparison among the perforation rates of Maloney,
balloon, and savary dilation of esophageal strictures. Gastrointest Endosc 2000; 51:460.
16.
RISK FACTORS
• Alarge hiatal hernia
• A history of previous esophageal
perforation
• A history of prior esophageal surgery
(such as for trauma or a congenital
abnormality)
Boerhaave syndrome
• Itis thought to occur due to a forceful ejection of
gastric contents in an unrelaxed oesophagus
against a closed glottis.
• Also due to sudden rise in intra-esophageal
pressure with negative intrathoracic pressure e.g.
after forceful vomiting,
retching,seizures,childbirth,heavy lifting
• Typically affects distal left posterolateral esophagus.
19.
Boerhaave syndrome
• Itis named after Hermann Boerhaave
(1668-1738),a Dutch professor of clinical
medicine .
• The syndrome was described after
the case of Dutch Admiral Baron
Jan von Wassenaer, who died of
the condition in 1723.
20.
Boerhaave syndrome
• Thefirst successful repair of post-
emetic esophageal rupture was
performed by Barrett in 1946.
21.
Boerhaave syndrome
• Thetears are vertically oriented,1-4 cm in length.
• Approximately 90% occur along the left
posterolateral wall of the distal esophagus,3-6
cm above the esophageal hiatus of the
diaphragm
• Complete disruption of wall in the absence of
preexisting pathology
• Male and alcoholic are more prone.
22.
BOERHAAVE’S SYNDROME
TRIAD
• Incase of Boerhaave’s Syndrome patient
may presented with the clinical triad
Mackler's
triad
Vomiting
Subcutaneous
emphysema
Chest pain
23.
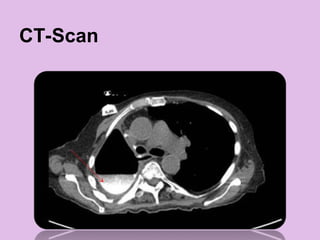
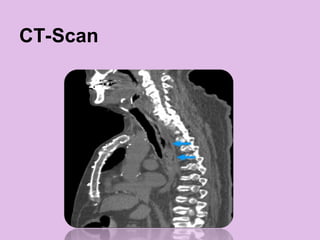
CLINICAL PRESENTATION
• Theclinical features of esophageal
perforation depend upon the location of
the perforation, degree of leakage, and the
duration since the injury.
24.
CLINICAL PRESENTATION
<24hrs
Cervical perforation
•Neck pain
• Tenderness over sternocleidomastoid
• Movement of the thyroid cartilage often elicit
significant pain
• Dysphonia
• Hoarseness
• Cervical subcutaneous emphysema
INITIAL MANAGEMENT
•ICU carewith close monitoring
•NPO + enteral feeding distal to perforation (jejunal)
or parenteral
•Fluid resuscitation
•Broad spectrum I/V antibiotics
•Opiate based analgesics
•Proton pump inhibitor
•Monitors Vitals
•Tube thoracostomy
•Preparation for operative management
37.
PRINCIPLES OF SURGICAL
MANAGEMENT
•Primary repair of the perforation site is the
optimal procedure
• Best if diagnosis is within 24 hours and
tissue is healthy
.
38.
PRINCIPLES OF SURGICAL
MANAGEMENT
•Exceptions to performing a primary repair
Cervical perforation that cannot be accessed but can
be drained
Diffuse mediastinal necrosis
Perforation too large for the esophagus to be re-
approximated
Esophageal malignancy
Pre-existing end-stage benign esophageal disease
(eg, achalasia)
The patient is clinically unstable
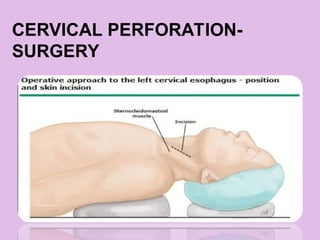
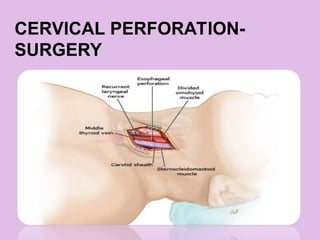
CERVICAL PERFORATION-
SURGERY
• Moreeasily treated
• Primary repair performed if the perforation site
clearly visualized and if there is no distal
obstruction
• Otherwise drainage of the perforation is adequate
to control leak since the anatomical structure of
the neck typically confine extraluminal
contamination to a limited space and thereby
enhance spontaneous healing
THORACIC ESOPHAGEAL
PERFORATION -SURGERY
• Mid-esophageal perforation is approached
through a right thoracotomy at the sixth or
seventh intercostal space.
• Distal esophageal perforation is
approached through a left thoracotomy at
the seventh or eighth intercostal space
POSTOPERATIVE
MANAGEMENT
• Nutritional supportis necessary until oral
feedings can be initiated and effectively
sustained.
• The patient is maintained on intravenous
broad spectrum antibiotics typically for 7 to
10 days.
47.
POSTOPERATIVE
MANAGEMENT
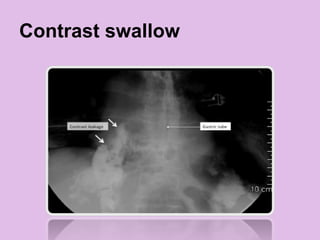
• Contrast esophagogramis obtained on 7th
POD if the patient is clinically stable.
• Drains remain in place until patient is
tolerating oral feedings and without clinical
evidence of a leak.
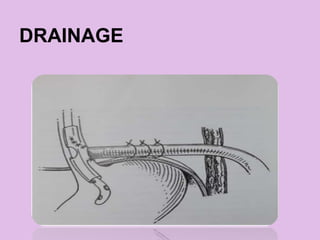
DRAINAGE
• Surgical drainageas the sole operative
management is reserved for perforations of
the cervical esophagus when the perforation
site cannot be completely visualized and
when there is no distal obstruction.
• T-tube may be inserted into the perforation to
create a controlled fistula when a patient
cannot tolerate more extensive surgery.
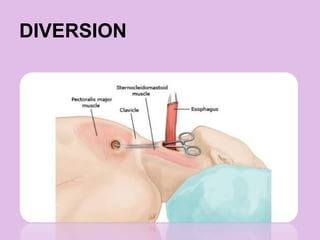
DIVERSION
• The patientis unstable
• The defect is large due to tissue
destruction from contamination
• Pre-existing esophageal disease is
present
52.
DIVERSION
• The goals
Controland drain extraluminal
contamination
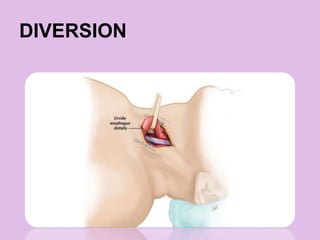
Divert the esophagus proximally with a
cervical esophagostomy
Resection of the remaining esophagus
53.
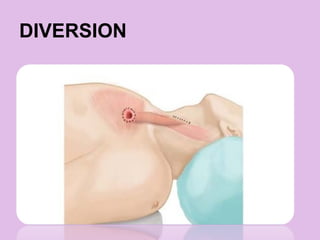
DIVERSION
• The goals
Obtaingastric diversion with a
gastrostomy tube and feeding tube
access with a jejunostomy
Close the diaphragmatic hiatus
INDICATIONS IN SURGICAL
MANAGEMENTS
•A primary repair is the gold standard of
care
• Drainage alone should only be performed
for perforation of the cervical esophagus
when the perforation cannot be visualized
and when there is no distal obstruction.
60.
CONTD,
• Diversion isreserved for patients who present with
clinical instability and where more extensive
operative procedure is not possible or when
extensive esophageal damage precludes a primary
repair.
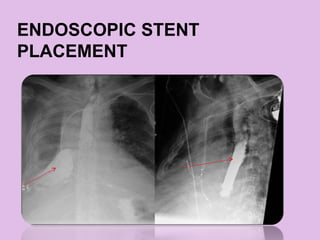
• Esophageal stents may be appropriate for patients
with extensive comorbidities, advanced mediastinal
sepsis, or large esophageal defects and the
patient’s inability to tolerate more extensive surgery.
61.
ESOPHAGECTOMY
• A primaryrepair alone of an esophageal
perforation should not be performed…
Proximal to untreated achalasia,
An undilatable stricture, or
In malignancy
62.
CONTD
• Esophagectomy shouldbe performed when the
patient presents with malignancy, extensive
esophageal damage that precludes repair, or end-
stage benign esophageal disease.
• Non-operative management should be reserved for
clinically stable patients with no evidence of systemic
inflammation, expediently diagnosed perforations,
and no spillage of mediastinum, pleura or
peritoneum.
63.
OUTCOMES FOLLOWING
OPERATIVE MANAGEMENT
•The principal variables associated
with mortality
Delay in diagnosis
Type of repair
Location of perforation
Etiology of the perforation
64.
SUMMARY
• Prompt diagnosisand management is
critical to minimizing mortality.
• The mortality rate following operative
management of an esophageal perforation
is dependent on location of the perforation.