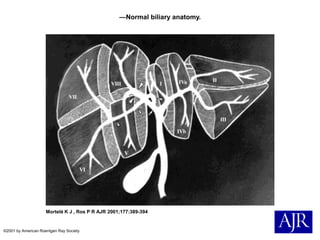
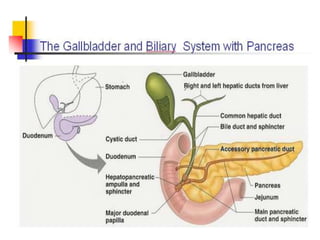
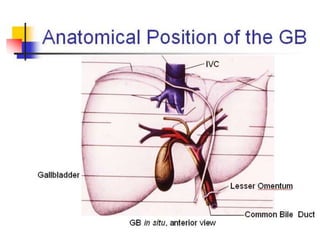
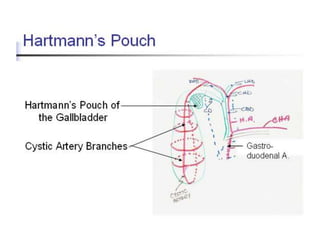
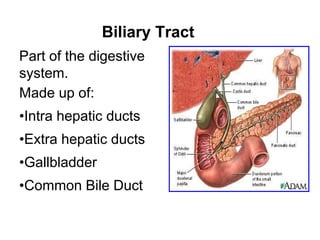
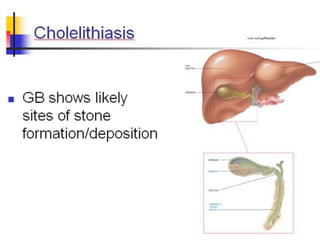
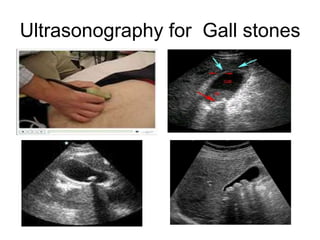
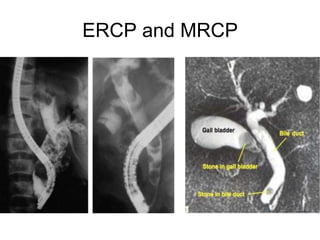
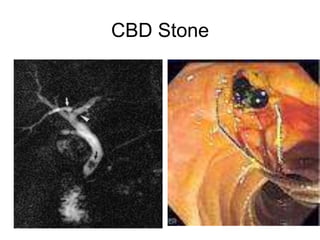
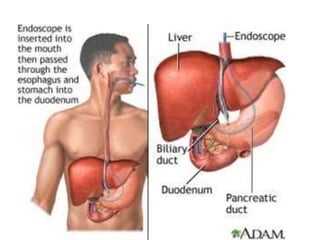
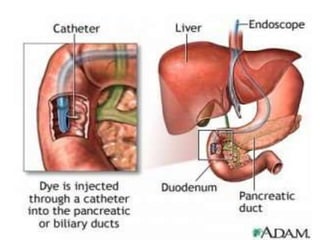
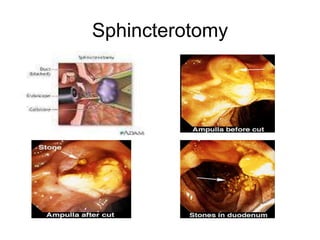
The document describes the anatomy and pathologies of the biliary tree. It is made up of the intrahepatic and extrahepatic bile ducts, gallbladder, and common bile duct. Common conditions covered include gallstones, biliary tract tumors, acute acalculous cholecystitis, Mirizzi's syndrome, and primary biliary disorders. Investigations like ultrasound and MRCP are used to diagnose conditions like gallstones, tumors, and bile duct stones. Treatments involve cholecystectomy for gallstones or tumors as well as ERCP for bile duct stone removal or stenting of bile duct cancers.



















![Surgery cholangitis[1]](https://cdn.slidesharecdn.com/ss_thumbnails/surgery-cholangitis1-120601032247-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)




























