Post partum hemorrhage
Postpartumhemorrhage is defined as
blood loss of >500 mL following vaginal
delivery & >1000 mL following a cesarean
section.
It can also be defined as blood loss that
results in hemodynamic instability.
The incidence of PPH is about 5% of all
pregnancies.
3.
PPH is dividedinto:
• Primary PPH: Bleeding occurring
within 24 hours of delivery.
• Secondary PPH: Bleeding occurring
after 24 hours but before 12 weeks
of delivery.
4.
• Minor PPHif the blood loss is 500 - 1000 mL
• In practice, blood losses between 500 &
1000 mL are relatively common, & can
usually be tolerated well by the woman.
• Major obstetric haemorrhage is defined as
blood loss ≥ 2,500 ml, or requiring a blood
transfusion ≥5 units red cells or treatment
for coagulopathy.
Diagnosis
• Early recognitionof blood loss & rapid action is
vital in the management of PPH.
• Appreciation of risk factors.
• Accurate estimation of blood loss & recognition of
the maternal signs of hypovolemia, These include
• Tachycardia,
• Low blood pressure,
• Symptoms of nausea, vomiting & feeling faint,
• pallor & slow capillary refill (>2 seconds).
7.
How should PPHbe managed?
management involves four components,
all of which must be undertaken
SIMULTANEOUSLY:
1) Communication.
2) Resuscitation.
3) Arresting the bleeding.
4) Monitoring and investigation.
Resuscitation
• A: Assessairway.
• B: Oxygen by mask at 10–15 litres/minute.
• C: 2 I.V lines 20 ml blood sample for FBC,
coagulation screen, urea, electrolytes &
cross match (4 units).
• Position flat & Keep the woman warm
• Transfuse blood as soon as possible.
• Until blood is available, infuse warmed
crystalloid /or colloid
10.
.
• If crossmatched blood is still unavailable, give
O-NEGATIVE blood
• FFP 4 units for every 6 units of red cells or PT
APTT> 1.5 x normal
• Platelets concentrates if PLT count < 50 x 109
• Cryoprecipitate If fibrinogen < 1 g/l.
Pharmacological measures
• Syntocinon5 units slow i.v (may have repeat dose).
• Ergometrine 0.5 mg by slow i.v or i.m (CI)
• Syntocinon infusion (40 units in 500ml fluid at
125ml/hour)
• Carboprost 0.25 mg by IM injection repeated doses
may be needed
• Misoprostol 1000 micrograms rectally.
• If pharmacological measures fail to control the
haemorrhage, initiate surgical haemostasis sooner
rather than later.
Monitoring & investigations
•temperature every 15 minutes.
• Continuous vital signs monitoring(using
oximeter, electrocardiogram and automated
blood pressure recording).
• Foley catheter to monitor urine output.
• Consider transfer to ICU once the bleeding is
controlled.
• Documentation of fluid balance, blood,
blood products and procedures performed.
16.
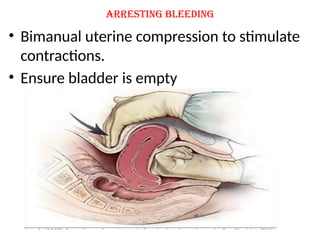
Secondary PPH: etiology
1-subinvolutionof uterus due to retained placental
tissue &/or endometritis
2-Lower genital tract laceration/ hematoma
3-Surgical injury
4-Dehiscence of CS scar
5-Coagulopathy/ bleeding disorder
6-gestational trophobastic disease.
Infection is the most common cause of post natal
morbidity between day 2 & day 10.
17.
Assessment
• History: Historyof offensive lochia,
abdominal cramping & maternal pyrexia is
often present
• Examination:
• general examination, fever, rigor, tachycardia
• abdominal palpation to assess uterine
involution &/or tenderness
• vaginal exam : speculum examination to see
if there’s any laceration.
18.
Investigations
• FBC
• C-reactiveprotein
• high vaginal swab
• USG in case of retained product of
conception.
• B-hcg
• duplex color Doppler
19.
Management
Antibiotics.
uterotonics.
evacuation of retained products of
conception
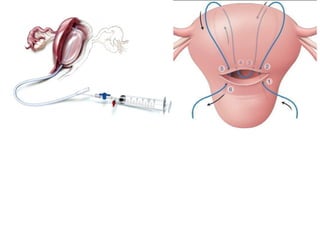
In continuing haemorrhage, insertion of
balloon catheter may be effective
Secondary PPH is often associated with
endometritis.
20.
• When antibioticsare clinically indicated, a
combination of ampicillin (clindamycin if penicillin
allergic) and metronidazole is appropriate. In
cases of endomyometritis (tender uterus) or overt
sepsis, then the addition of gentamicin is
recommended.
• Surgical measures should be undertaken if there is
excessive or continuing bleeding, irrespective of
ultrasound findings.
• A senior obstetrician should be involved in
decisions and performance of any evacuation of
retained products of conception as these women
are carrying a high risk for uterine perforation.
21.
Sudden maternal collapse
Maternalcollapse is defined as an acute
event involving the cardiorespiratory
systems and/or brain, resulting in a
reduced or absent consciousness, in
pregnancy & up to 6 weeks after delivery.
vasovagal attacks & the postictal state are
the most common causes of „maternal
collapse‟.
.
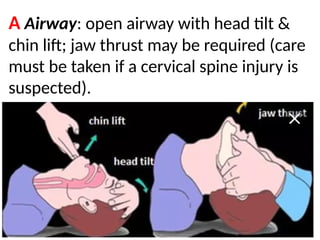
A Airway: openairway with head tilt &
chin lift; jaw thrust may be required (care
must be taken if a cervical spine injury is
suspected).
24.
.
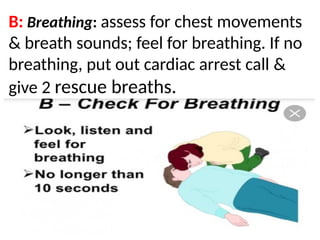
B: Breathing: assessfor chest movements
& breath sounds; feel for breathing. If no
breathing, put out cardiac arrest call &
give 2 rescue breaths.
25.
.
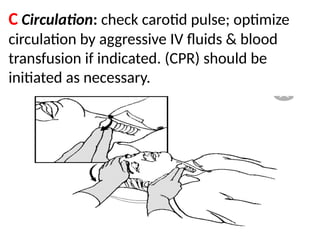
C Circulation: checkcarotid pulse; optimize
circulation by aggressive IV fluids & blood
transfusion if indicated. (CPR) should be
initiated as necessary.
.
• D Drugs:to maintain circulation, combat
infection, antidotes if drug overdose,
anticoagulants in cases of massive embolism.
• E Environment: avoid injury (eclampsia),
ensure safety of patient and staff.
• F Fetus: if CPR is required at >20wks, unless
there is immediate reversal, immediate CS (at
the location of the arrest) must be
performed. If CPR is not required, assess fetal
well-being and plan delivery as appropriate
once maternal condition is stable.
28.
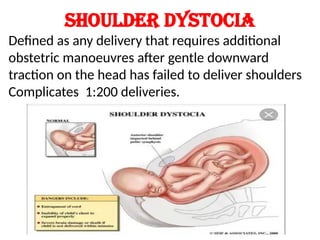
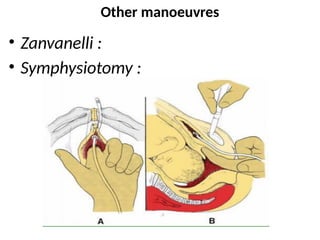
Shoulder dystocia
Defined asany delivery that requires additional
obstetric manoeuvres after gentle downward
traction on the head has failed to deliver shoulders
Complicates 1:200 deliveries.
30.
HELPERR
• H Callfor help (including midwifes, senior
obstetrician, neonatologist, anaesthetist).
31.
.
• E Episiotomy—remembershoulder
dystocia is a bony problem, but an
episiotomy may help with internal
manoeuvres.
32.
.
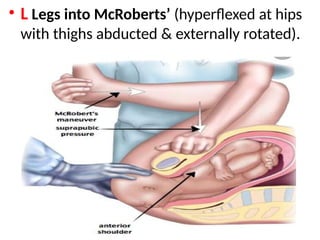
• L Legsinto McRoberts’ (hyperflexed at hips
with thighs abducted & externally rotated).
33.
.
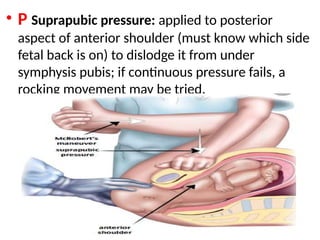
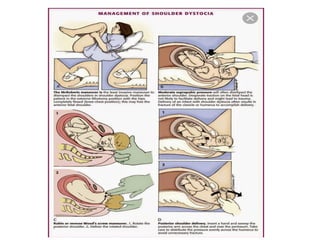
• P Suprapubicpressure: applied to posterior
aspect of anterior shoulder (must know which side
fetal back is on) to dislodge it from under
symphysis pubis; if continuous pressure fails, a
rocking movement may be tried.
34.
.
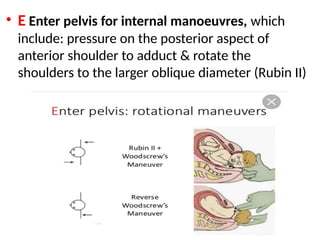
• E Enterpelvis for internal manoeuvres, which
include: pressure on the posterior aspect of
anterior shoulder to adduct & rotate the
shoulders to the larger oblique diameter (Rubin II)
35.
.
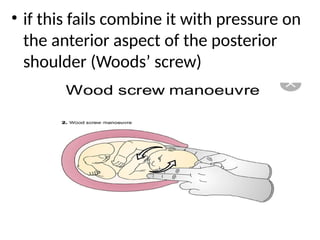
• if thisfails combine it with pressure on
the anterior aspect of the posterior
shoulder (Woods’ screw)
36.
.
If this fails,reversing manoeuvre may
be tried with pressure on the anterior
aspect of anterior shoulder and
posterior aspect of posterior shoulder
in opposite direction (reverse Woods’
screw).
37.
.
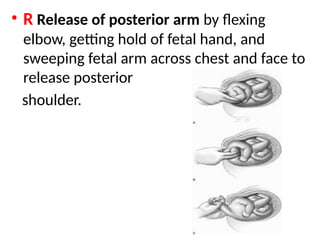
• R Releaseof posterior arm by flexing
elbow, getting hold of fetal hand, and
sweeping fetal arm across chest and face to
release posterior
shoulder.
.
• R Rollover to ‘all fours’ may help aid
delivery by the changes brought about in
the pelvic dimensions (Gaskin manoeuvre).
In practice, 80% of babies will deliver with
suprapubic pressure & McRoberts’
manoeuvre. If these fail, delivery of posterior
arm is probably the best next manoeuvre.
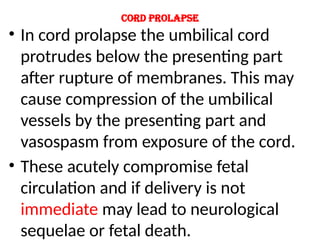
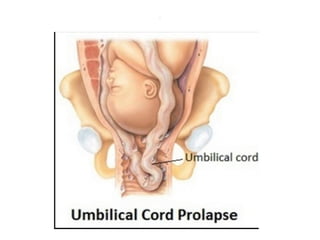
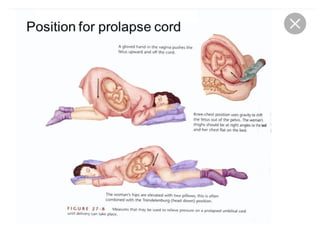
Cord prolapse
• Incord prolapse the umbilical cord
protrudes below the presenting part
after rupture of membranes. This may
cause compression of the umbilical
vessels by the presenting part and
vasospasm from exposure of the cord.
• These acutely compromise fetal
circulation and if delivery is not
immediate may lead to neurological
sequelae or fetal death.
Management
• The fetusshould be delivered as rapidly
as possible; this may be by instrumental
delivery or category 1 CS.
• Prevent further cord compression
during transfer for CS by:
1. knee-to-chest position
.
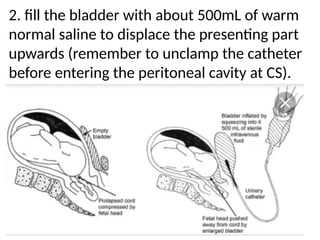
2. fill thebladder with about 500mL of warm
normal saline to displace the presenting part
upwards (remember to unclamp the catheter
before entering the peritoneal cavity at CS).
47.
.
3. A handin the vagina to push up the
presenting part (may not always be
practical).
48.
.
• Prevent spasmby avoiding exposure of cord.
Reduce cord into vagina to maintain body
temperature & insert a warm saline swab to
prevent cord coming back out.
• It is important to avoid handling the cord as
this provokes further spasms.
• Tocolytics may be administered to abolish
uterine contractions & improve oxygenation
to the fetus may cause PPH at CS due to
uterine atony.
• Neonatal team must be present at delivery.
49.
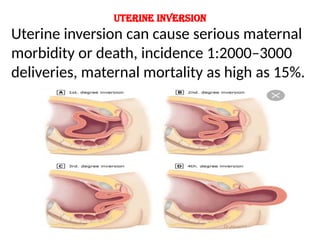
Uterine inversion
Uterine inversioncan cause serious maternal
morbidity or death, incidence 1:2000–3000
deliveries, maternal mortality as high as 15%.
50.
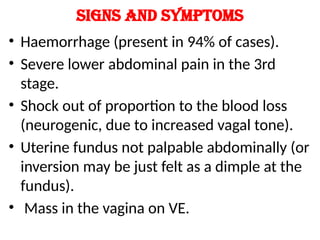
Signs and symptoms
•Haemorrhage (present in 94% of cases).
• Severe lower abdominal pain in the 3rd
stage.
• Shock out of proportion to the blood loss
(neurogenic, due to increased vagal tone).
• Uterine fundus not palpable abdominally (or
inversion may be just felt as a dimple at the
fundus).
• Mass in the vagina on VE.
51.
Management of uterineinversion
Call for help (including a senior obstetrician
and anaesthetist).
52.
.
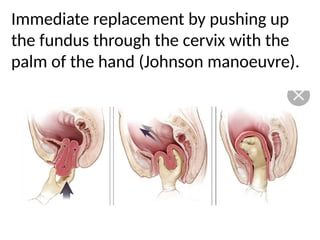
Immediate replacement bypushing up
the fundus through the cervix with the
palm of the hand (Johnson manoeuvre).
53.
.
• Bloods forFBC, coagulation studies, & cross-
match 4–6U.
• Immediate fluid replacement.
• Continuous monitoring of vital signs.
• Transfer to theatre & arrange appropriate
analgesia.
• If the placenta is still attached to the uterus it is
left in situ to minimize the bleeding, & removal
attempted only after replacement.
• Tocolytic drugs, such as terbutaline, or volatile
anaesthetic agents may be tried to make
replacement easier.
54.
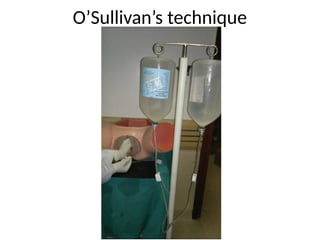
.
• If manualreduction fails then hydrostatic
repositioning (O’Sullivan’s technique) may
be tried:
• warm saline is rapidly infused into the
vagina with one hand, sealing the labia (a
silicone ventouse cup may be used to
improve seal)
• uterine rupture should be excluded first.





















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

