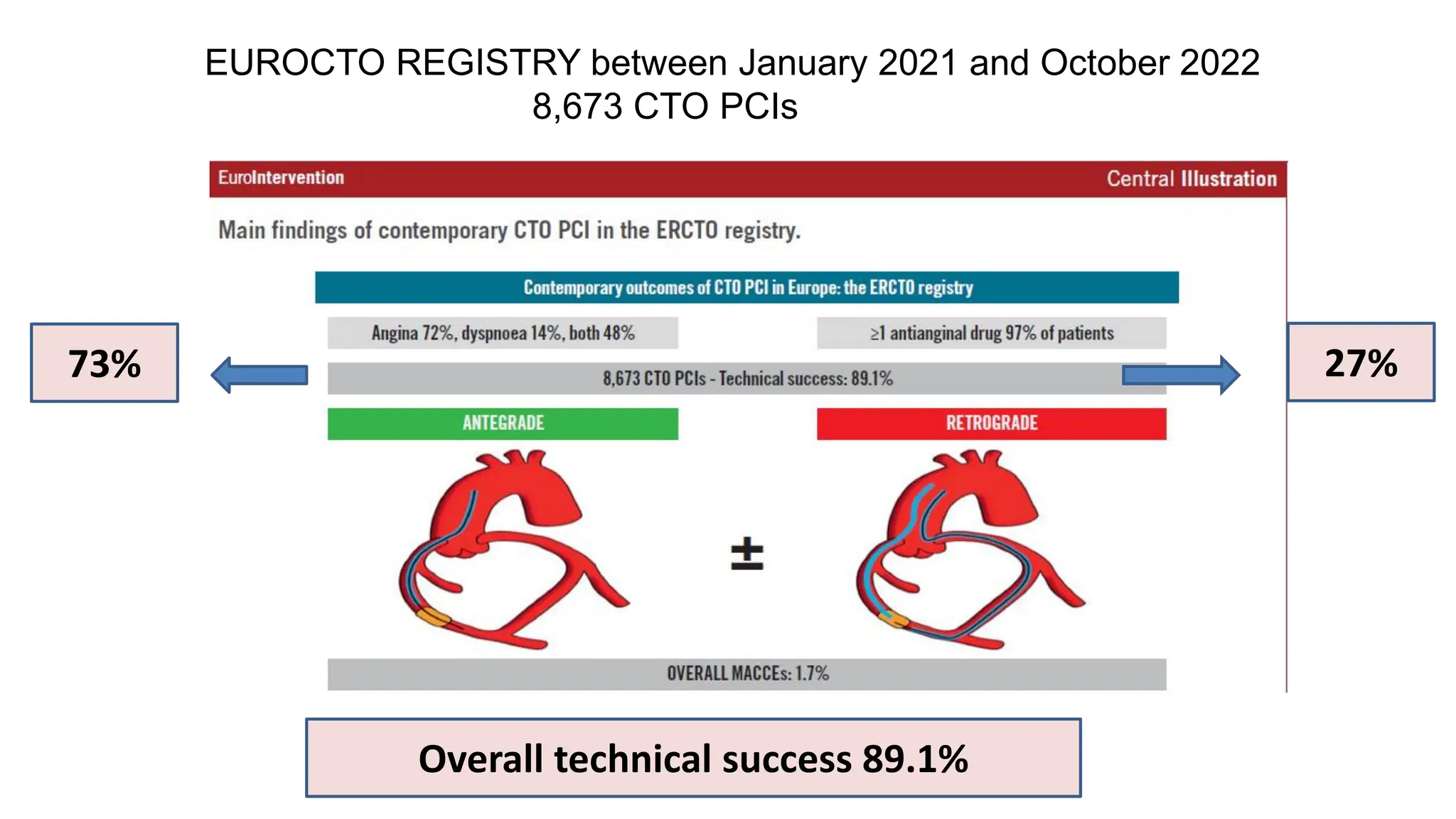
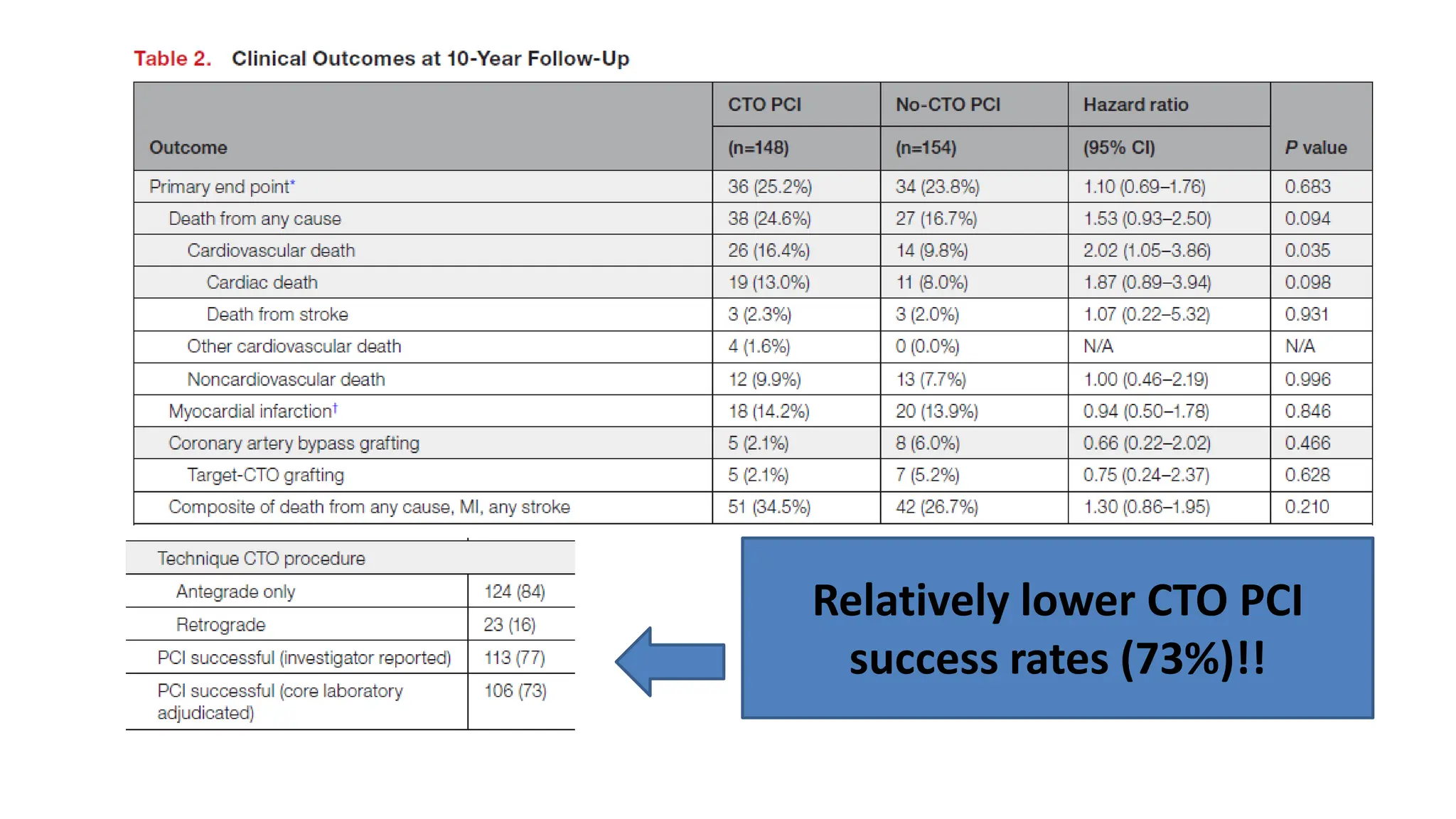
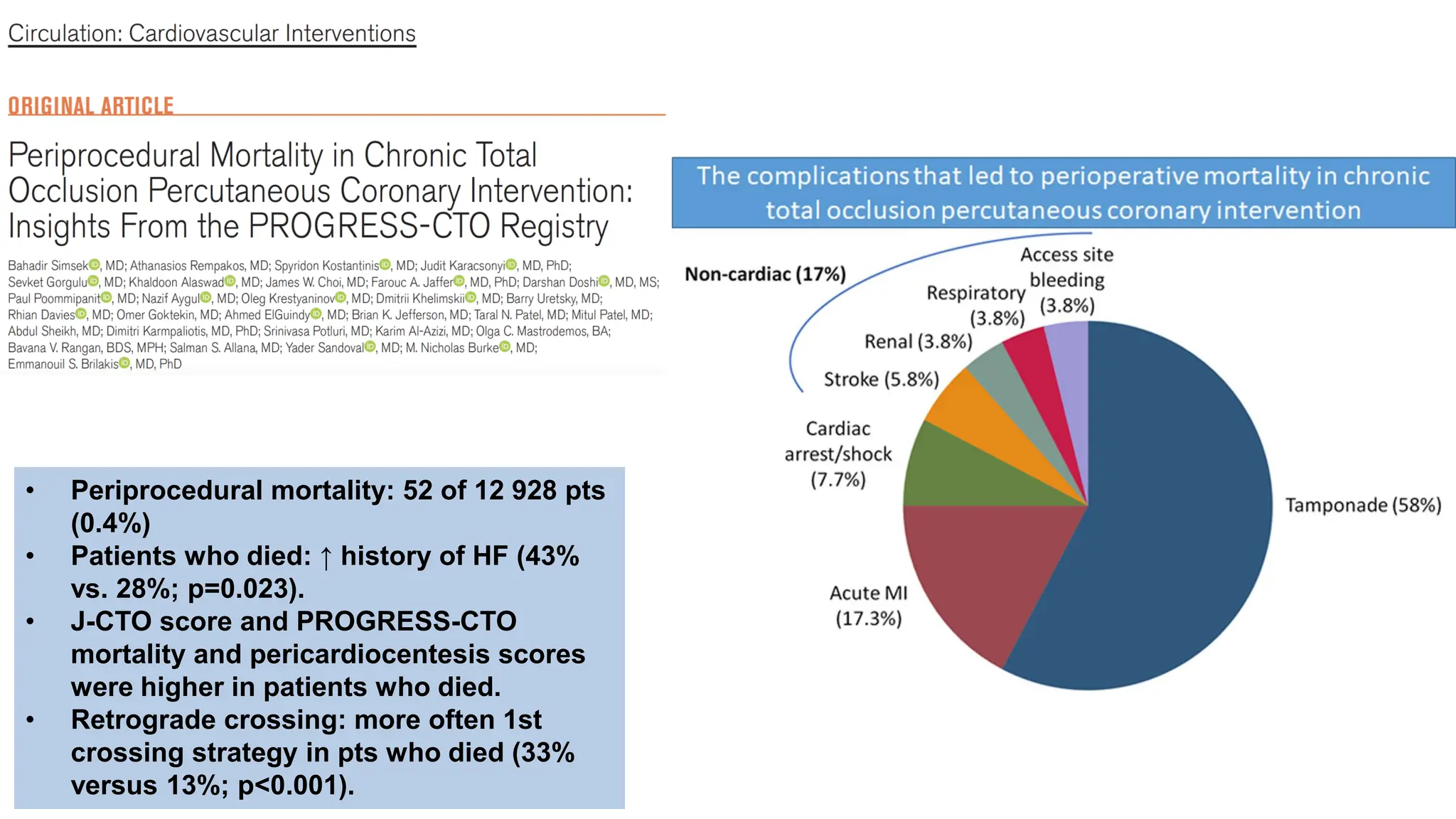
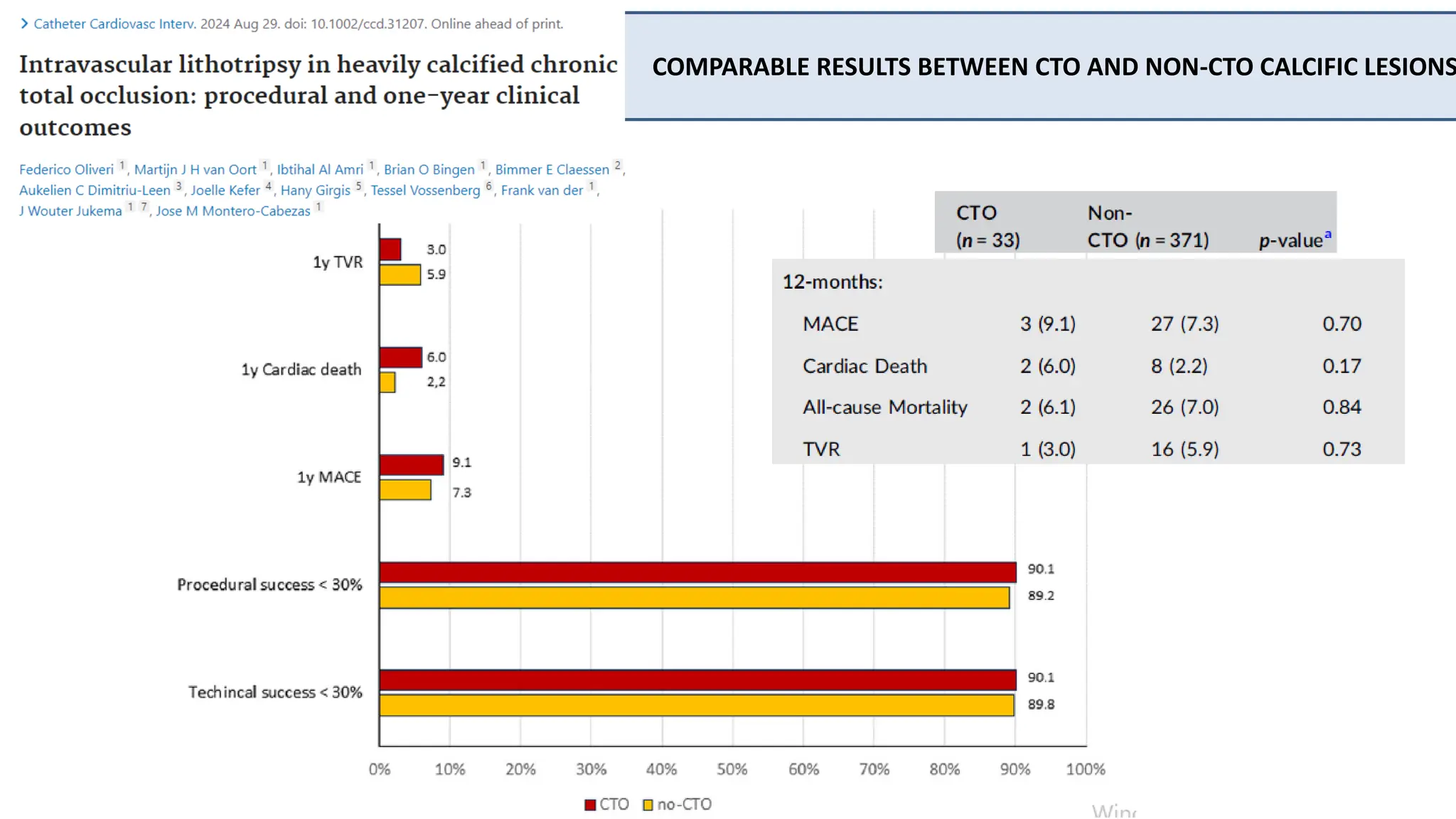
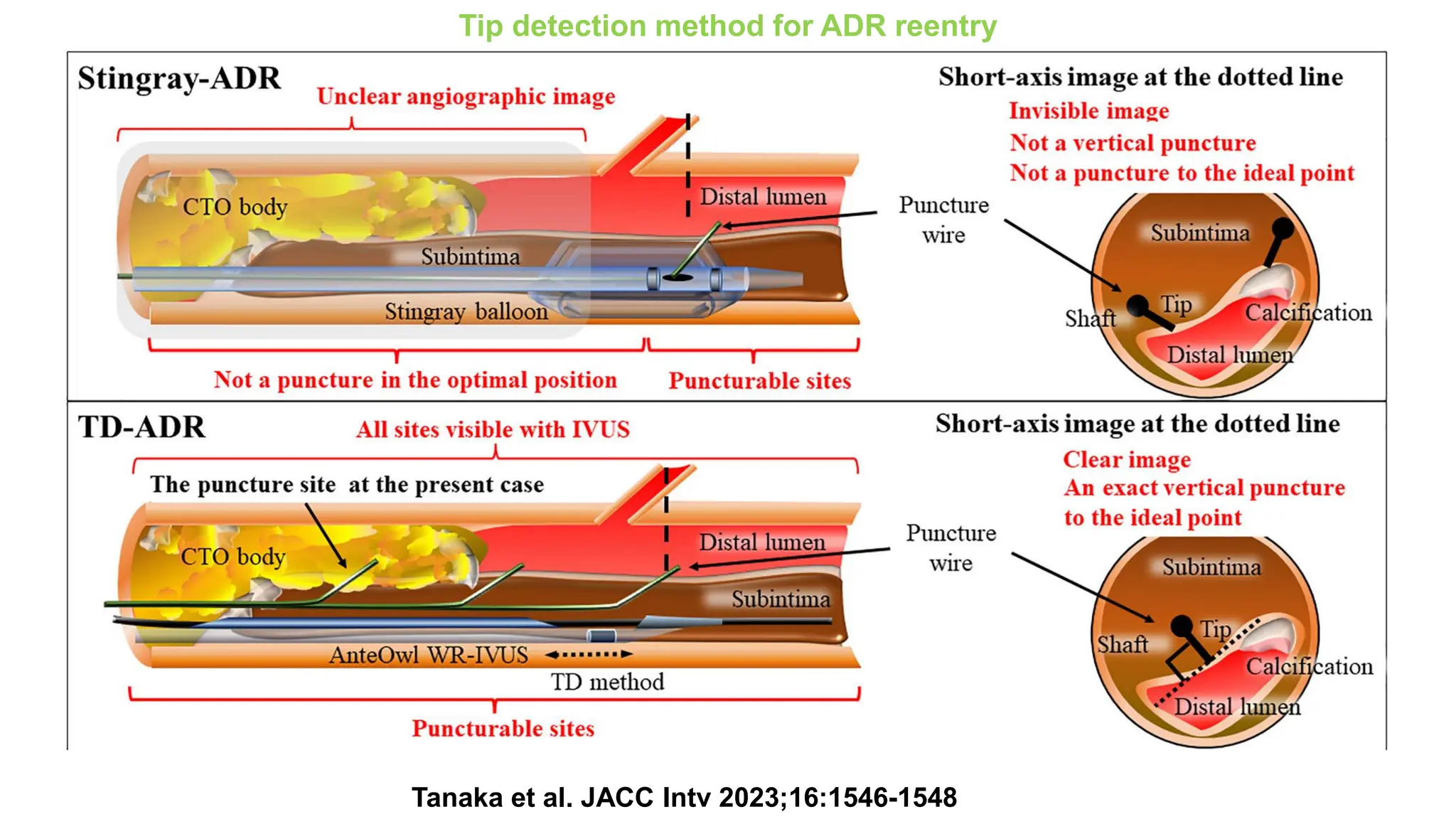
The document provides an overview of coronary chronic total occlusion (CTO) publications and studies, detailing technical success rates, risk factors, and outcomes associated with CTO percutaneous coronary interventions (PCI). Key findings include varying success rates based on lesion characteristics, operator volume, and treatment approaches, with a focus on follow-up data indicating potential benefits of specific strategies. Additionally, it discusses the prevalence of burnout among interventional cardiologists involved in CTO procedures and highlights the need for standardized methods in the field.