Definition
Nursing process isa critical thinking process that professional
nurses use to apply the best available evidence to caregiving and
promoting human functions and responses to health and illness
(American Nurses Association, 2010).
A Process: Is a method for organizing and delivering nursing care.
Is a series of steps or components leading to the achievement of a goal
3.
• Nursing processis a systematic method of providing care to clients.
• The nursing process is a systematic method of planning and providing
individualized nursing care.
4.
Purposes of nursingprocess
• To identify a client’s health status and actual or potential health care
problems or needs.
• To establish plans to meet the identified needs.
• To deliver specific nursing interventions to meet those needs.
• Evaluate the effectiveness of Nursing Care in achieving client goals
5.
Components of nursingprocess
•It involves assessment (data collection), nursing
diagnosis, planning, implementation, and
evaluation.
Characteristics of NursingProcess
• Dynamic nature,
• Client centeredness
• Focus on problem solving and decision making
• Interpersonal and collaborative style
• Use of critical thinking and clinical reasoning.
Definition
Assessment is thesystematic and continuous collection, organization,
validation, and documentation of data (information).
Is the process of gathering, verifying and communicating data about a client
11.
Purpose of Assessment:
•Is to establish a database about:
1. Client's level of wellness
2. Health practices
3. Past illnesses & related experiences
4. Health Care goals
• This data is the basis for an individualized plan of nursing care.
12.
•Data includes:
•1. NursingHealth History
•2. Physical Examination
•3. Results of laboratory & diagnostic examination
•4. Information from health care team members
•5. Client's family
13.
Data Collection:
• Datacollected should be:
• 1. Descriptive: Client's perception of a symptom
Perceptions and observations of the family Nurse's
observation Reports from other members of health team
• 2. Conciseموجز: Describe the information obtained
• 3. Complete: Nurse obtains all information relevant to the
actual or potential health problem
14.
Types Of Data
•1. Subjective Data: Client's perceptions about his health problem
• Example: Presence of Pain (Frequency, Duration, Location and Intensity)
• Subjective data usually include:
Feelings of anxiety
Physical discomfort
Mental stress
• 2. Objective Data: Observations or Measurements made by the data
collector
Example: Observations (Identifying the presence of actual body
rash)Measured (Hyperthermia, head circumference, elevated blood
pressure, tachycardia)
15.
Sources Of Data
.1Client: The best source of information.
The client can provide the most accurate information about:
Health care needs Present and past illnesses Lifestyle pattern Perception of
symptoms • Changes in activities of daily living
2 .Family: The primary sources of information about infants or children and
critically ill, mentally , disoriented or unconscious client.
In cases of severe illness or emergency situations, families maybe the only
source of data about client's health-illness patterns, current medications,
allergies, onset of illness and other information needed by nurses and
physicians.
3. Health Care Team Members: They can provide data about the way the client
interacts within the health care environment, reacts to information about
diagnostic tests, and responds to visitors.
4. Medical Records: It can verify information about past health patterns and
treatment or can provide new information.
5. Other Records
16.
Methods Of DataCollection
• 1. Interview
• 2. Nursing Health History
• 3. Physical Examination
• 4. Results Of Laboratory & Diagnostic Tests
17.
Interview
It is thefirst step in collecting the subjective information.
Purposes of Interview:
a. To obtain a nursing health history
b. Identify health needs & risk factors
c. Determine specific changes in level of wellness & pattern of living
The Interviewer obtains information about the:
d. Client's Health State
e. Lifestyle
f. Support Systems
g. Patterns of Illness
h. Patterns of adaptation, strength, and limitations, and resources
18.
The Nursing HealthHistory
• The data collected about:
1. The client level of wellness
2. Changes in Life Patterns
3. Socio-cultural Role
4. Mental and emotional reactions to illness
Objectives Of Nursing History
5. To identify patterns of health & illness
6. To identify risk factors for physical & behavioral health problems
7. Available resources for adaptation
Data should be collected about client's Physical, Developmental,
Intellectual, Emotional Social & Spiritual dimensions
19.
Present Illness
• Ifillness is present, nurses gather essential data and relevant data
about:
• 1. Onset of symptoms (sudden or gradual)
• 2. Whether symptoms are always present or come and go
• 3. Duration of symptoms
• 4. Location, intensity & quality of symptoms
• 5. Actions that precipitates the symptoms, makes them worse or
provides relief
• 6. Client's expectations of the health care provided
20.
Past Medical History
•1. Previous hospitalizations
• 2. Previous surgery
• 3. Allergies (Food, drugs, Pollutants)
• 4. Use of alcohol, tobacco, caffeine or drugs or routinely taken
medications
• 5. Diseases involving the liver, lungs, heart
• 6. Patterns of sleep, exercise and nutrition
21.
Family History
• Todetermine whether the client is at risk for illnesses of a genetic or
familial nature
• .Example : cancer, heart disease, diabetes mellitus, kidney diseases,
hypertension or mental disorders.
22.
Environmental History
• Itincludes:
• 1. Exposure to pollutant that can affect health
• 2. High crime that prevents clients from walking around their
neighborhood.
•Psychosocial History
• It includes ways that the client and family cope with stressors
23.
• ■ ReviewOf Systems (Physical Examination)
• It is a systematic, method for collecting data on all body systems. The
nurse asks the client about the normal functioning of each system &
any noted changes.
• ■ Diagnostic And Laboratory Data
• Laboratory data are one more source of information the nurse uses in
completing a database. In addition to verify- ing abnormal findings
noted in the history & examination, laboratory data can identify
actual or potential health care problems not previously noted by the
client or examiner. Refer to table (2-1) A Guide to Common
Laboratory and Diagnostic Procedures.
24.
Validation of data
Theinformation gathered during the assessment is “double-
checked” or verified to confirm that it is accurate and complete.
After gathering the subjective & objective data, the data must be
validated to ensure its accuracy. The validation of each source of
assessment data is obtained by comparing the data with another
source.
Findings concerning physical examination & observation of client
behavior can be validated by comparing data in the medical record
with consultation form another health team member or family
member
25.
Documentation of data
Tocomplete the assessment phase, the nurse records
client data. Accurate documentation is essential and should
include all data collected about the client’s health status.
1. All data pertinent to client status are included, even
information that does not seem to indicate an abnormality
should be recorded
2. Observation & recording of client status is a legal and
professional responsibility. When recording data, a nurse
should pay attention to facts and should make an effort to be
as descriptive as possible.
Diagnosis: is thesecond phase interpret of the nursing process.
In this phase, nurses use critical thinking skills to assessment data
to identify client problems.
Diagnosis
29.
Nursing Diagnosis Process
•1. Data Analysis and Interpretation Example of Data Analysis.
• 2. Identification of client's problems Focusing on pertinent
assessment & abnormal data collected from
■ In describing health problems, the nurse moves from general to
specific
■ To identify client's need, the nurse first determines what the client's
health problems were & whether they re actual or potential problems
■ An Actual health problem is one that is perceived or experienced by
the client, such as "a sleep pattern disturbance related to a noisy
environment"
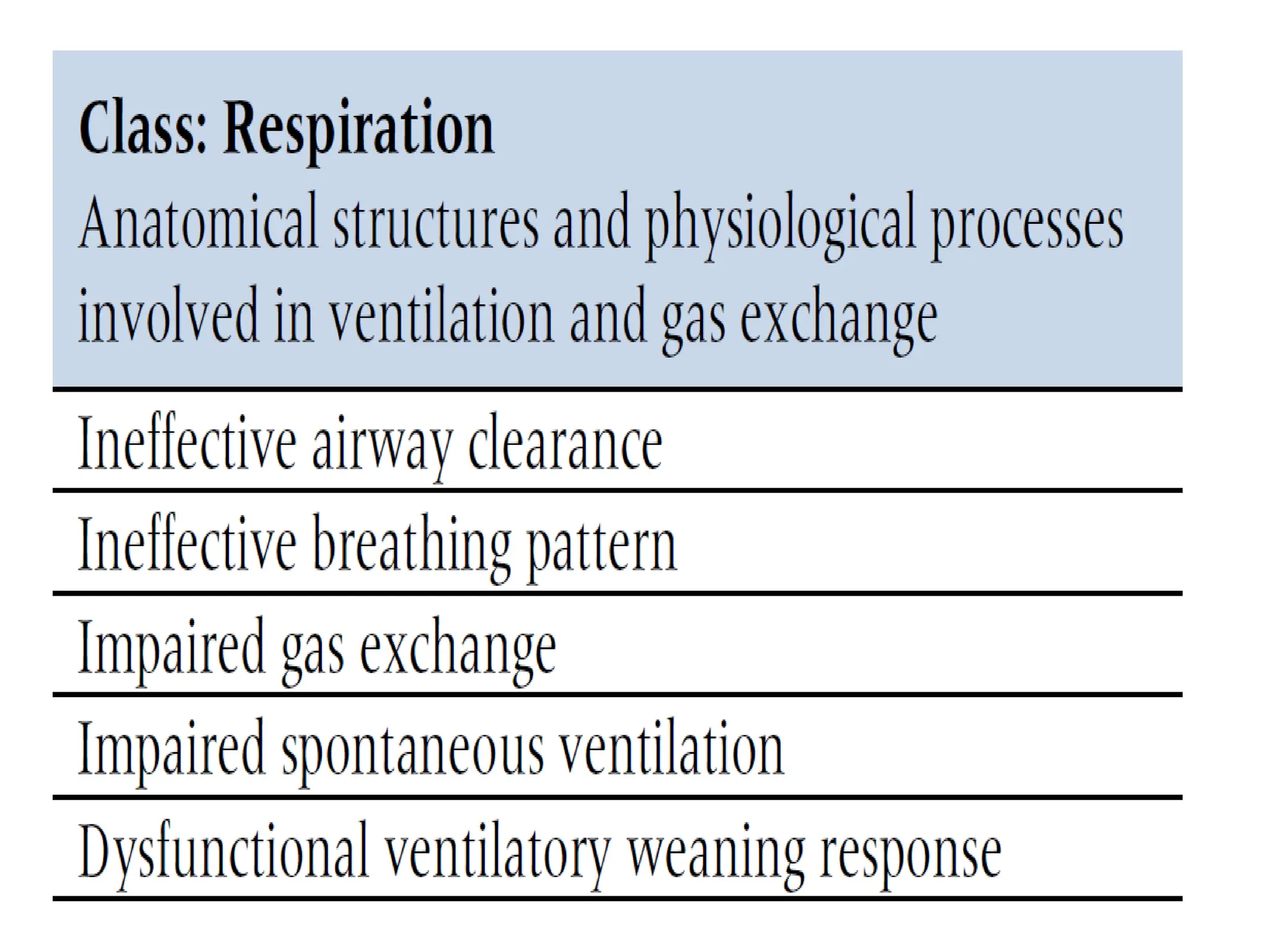
■ A Potential health problem is one for which the client is at risk, such
as an over weight smoker is at risk for ineffective airway clearance
related to incisional pain.
30.
Status of theNursing Diagnosis
The status of nursing diagnosis are actual, health promotion and risk.
1. An actual diagnosis is a client problem that is present at the time
of the nursing assessment.
2. A health promotion diagnosis relates to clients’ preparedness to
improve their health condition.
3. A risk nursing diagnosis is a clinical judgement that a problem
does not exist, but the presence of risk factors indicates that a
problem may develop if adequate care is not given.
31.
Example of dataAnalysis:
• Recognized patterns (possible defining characteristics):
■No bowel movement for 4 days
■ Painful defecation with straining
■Last stool small & hard
■ Abdomen firm and distended
• Compared with normal standards:
■ Soft, formed stool daily
■ Defecation not painful
■ Abdomen soft, non distended
• Make a reasoned conclusion:
■ Bowel elimination problem
32.
Components of aNANDA
Nursing Diagnosis
A nursing diagnosis has three components:
(1) The problem and its definition
(2) The etiology
(3) The defining characteristics.
33.
1. The problemstatement describes the client’s
health problem.
2. The etiology component of a nursing
diagnosis identifies causes of the health
problem.
3. Defining characteristics are the cluster of
signs and symptoms that indicate the
presence of health problem.
34.
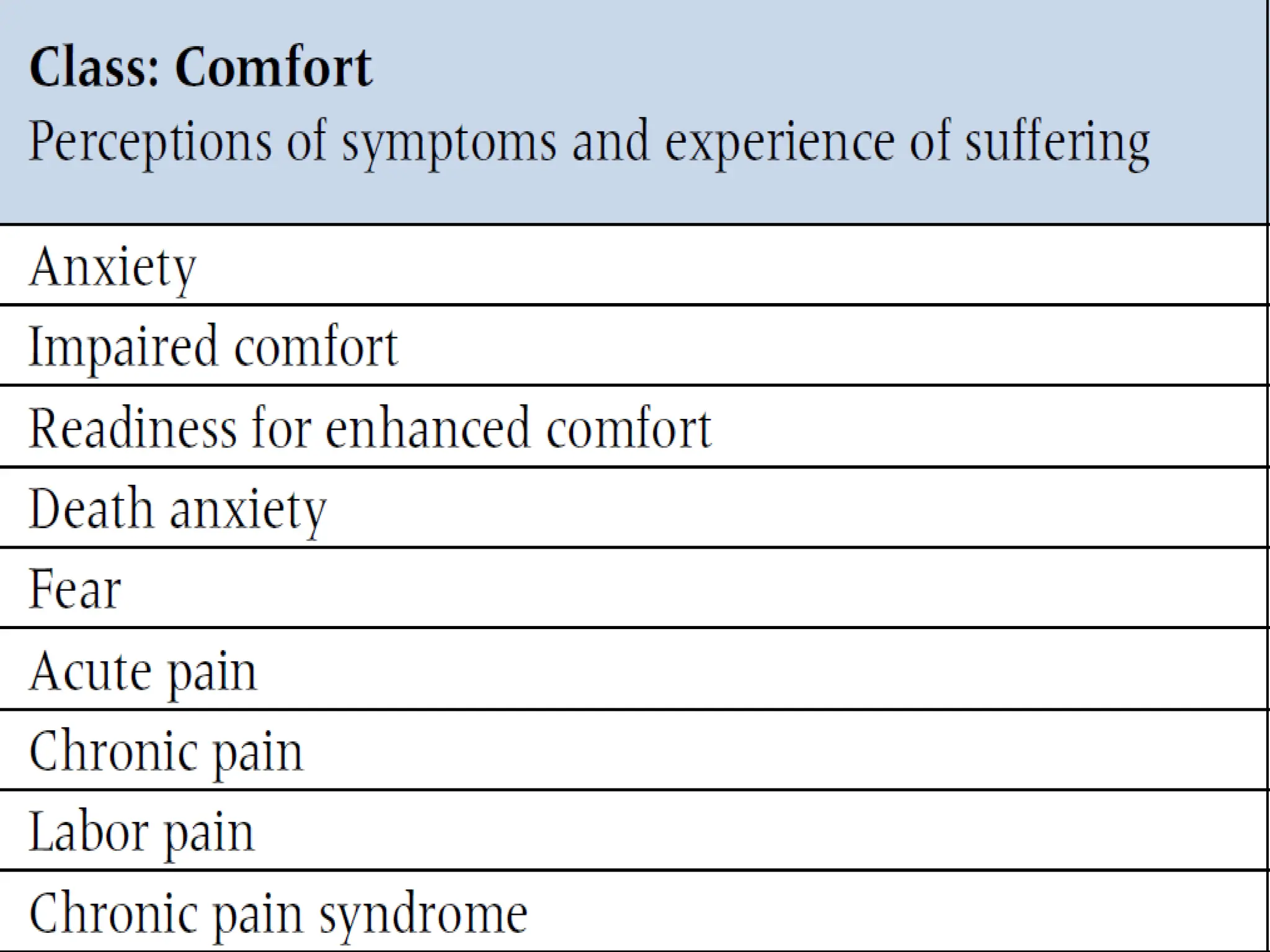
Acute pain relatedto
abdominal surgery as
evidenced by patient
discomfort and pain scale.
Problem Etiology Signs and symptoms
Pain Surgery of abdomen Pain scale and
discomfort of patient
Differentiating Nursing Diagnosis
fromMedical Diagnosis
Nursing diagnosis Medical diagnosis
A nursing diagnosis is a statement of
nursing judgment that made by nurse, by
their education, experience, and
expertise, are licensed to treat.
A medical diagnosis is made by a
physician.
Nursing diagnoses describe the human
response to an illness or a health
problem.
Medical diagnoses refer to
disease processes.
Nursing diagnoses may change as the
client’s responses change.
A client’s medical diagnosis
remains the same for as long as
the disease is present.
Planning
•involves decision makingand problem solving.
•It is the process of formulating client goals and
designing the nursing interventions required to
prevent, reduce, or eliminate the client’s health
problems.
58.
Establishing Priorities
Afterformulating specific nursing diagnosis, the nurse establishes
the priorities of the diagnosis by ranking them in order of
importance االهمية حسب
Priorities of care are established to identify the order in which
nursing interventions will be provided when an individual has
multiple problems or alterations.
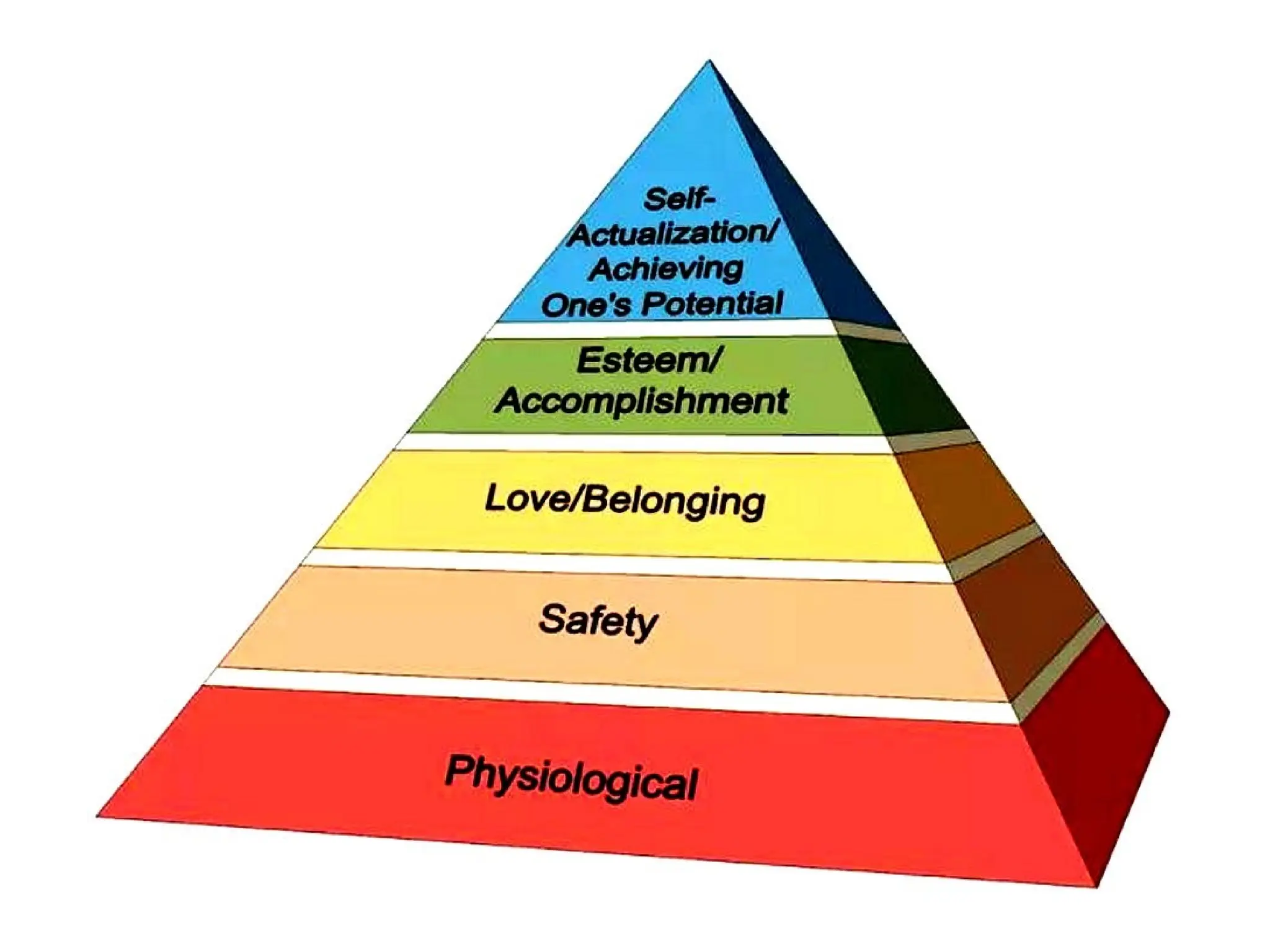
Maslow's hierarchy of needs can be useful in designating priorities
Basic physiological needs are given priority over safety needs
The needs for love, esteem and self-actualization may have a
lower priority
High priority must be given to psychological, sociocult- ural,
developmental or spiritual needs of the client
61.
Priorities Are Classified:
•1.High- Nursing diagnosis that if untreated, could
result in harm to the client or others have the
highest priority. (Diarrhea )
•2. Intermediate- nursing diagnosis involves the non-
emergency, non-life threatening needs of the
clients.(nutrition )
•3. Low- Nursing diagnosis are client's needs that
may not be directly to a specific illness or
prognosis(chronic infections due to hx of smoking
since 20 y)
62.
-
•Establishing Goals AndExpected Outcomes
After assessing, diagnosing, and establishing priorities about
client's health care needs, the nurse formulates goals &
expected outcomes with the client for each diagnosis.
63.
Types Of Goals:
•1. Short term goals: A short term goal is an objective that is expected
to be achieved in a short period of time, usually less than a week
A short-term goal for a client with ineffective airway clearance, for
example, maybe " Absence of abnormal lung sound within 2 days“
2. Long term goals: A long-term goal is an objective that is expected to
be achieved over a long period of time, usually over weeks or months.It
may be carried over into discharge, to skilled nursing facilities,
rehabilitation settings or return to the home.
For example: A long-term goal for a client with an effective airway
clearance maybe to "Remain free of upper respiratory infection for 6
months"
64.
These goals oftenfocus on
• :A) Prevention
• B) Rehabilitation
• C) Discharge &
• D) Health Education
Through goals, the nurse is able to provide continuity of care
& promote optimal use of time & resources
65.
Expected Outcomes:
• Anexpected outcome is the specific, step by step
objective that leads to attainment of the goal & the
resolution of the etiology of the nursing diagnosis.
•Outcomes are desired response of client condition
in the physiological, social, emotional
developmental or spiritual dimensions.
66.
Designing Nursing Interventions
•Thenurse uses assessment data, priority setting,
knowledge and experience to select actions that will
successfully meet the established goals & expected
outcomes.
•A nursing intervention is any treatment, that a nurse
performs to improve patient’s health.
67.
Types Of Interventions:
•1. Independent interventions involve aspects of professional
nursing practice, which require no supervision or direction from
others.
For example: Designing interventions for increasing a client's
knowledge about adequate nutrition, or activities of daily related
to hygiene is an independent nursing.
• 2. Interdependent; Example: Implementation of hypertension
protocol, in which the nurse has criteria to change drug or diet
therapies
• 3. Dependent; are based on the instruction or written orders
from other professionals.
68.
Writing Individualized Nursing
Interventions
•After choosing the appropriate nursing interventions, the nurse
writes them on the care plan.
• Nursing care plan is a written or computerized information about the
client’s care.
Implementation
•Implementation consists ofdoing and documenting
the activities.
•■ Implementation is category of nursing behavior in
which the actions necessary for achieving the expected
outcomes of nursing care are initiated & completed.
•In theory, implementation of the nursing care plan
follows the planning component of the nursing
process.
•In practice settings, implementation may begin directly
after assessment
71.
■ Immediate implementationis necessary when the
nurse identifies urgent needs of the client, such as:
a. A threat to physiological status
Example: Cardiac arrest
b. A threat to psychological status
Example: A sudden death of loved one
c. A threat to socio-economic status
d. A threat to spiritual status
Example: An illness viewed as God's punishment
72.
Implementing Nursing Interventions
•The nurse uses nursing interventions to achieve the goals of
care & selects from the following methods to achieve the goals
of nursing care:
1. Assisting in the performance of the activities of daily living
2. Counseling & educating the client & family
3. Give care to achieve therapeutic goals
4. Giving care to facilitate attainment of therapeutic goals by
the client
5. Supervising & evaluating the work of other staff members
• Evaluation isa planned, ongoing, purposeful activity in which
the nurse determines
(a) the client’s progress toward achievement of
goals/outcomes and
(b) the effectiveness of the nursing care plan.
75.
Evaluation
■ The evaluationcomponent of the nursing process measures
the client's response to nursing actions and the client's
progress towards achieving goals
■During evaluation, the nurse judges the success of the previous
steps of the nursing process by examining the client's responses &
comparing them with the behaviors stated in the expected outcomes
■ Another aspect of evaluation involves measurement of the
quality of nursing care provided in a health care setting and the
quality of care for a client
■ Quality assuranceضمان is an ongoing, systematic, comprehensive
evaluation of health care services & the impact of those on health
care consumers
Evaluations of nursing activities determine the types of nursing
actions performed and the level of success in achieving client goals.
It ensures quality professional nursing practice.
Writing The NursingCare Plan
• When using the five-column plan:
• 1. In the assessment column, the nurse includes all data relevant to
the corresponding nursing diagnosis.
• 2. In the nursing diagnosis column, the nurse includes all the
nursing diagnosis according to priority.
• 3. In the goal column, the nurse includes the previously developed
goals. At this point, the nurse begins to translate the short & long
term goals into action plans that anticipate the need of the client,
coordinates nursing care and select appropriate nursing, measures.
• 4. In the implementation column, the nurse writes the action plan
• 5. The evaluation column contains the projected outcome criteria
previously identified