November-December 2013 • Vol. 22/No. 6 359
Beverly Waller Dabney, PhD, RN, is Associate Professor, Southwestern Adventist University,
Keene, TX.
Huey-Ming Tzeng, PhD, RN, FAAN, is Professor of Nursing and Associate Dean for Academic
Programs, College of Nursing, Washington State University, Spokane, WA.
Service Quality and Patient-Centered
Care
L
eaders of the U.S. Depart -
ment of Health & Human
Services (2011) urge providers
to improve the overall quality of
health care by making it more
patient centered. Patient-centered
care (or person-centered care) refers
to the therapeutic relationship
between health care providers and
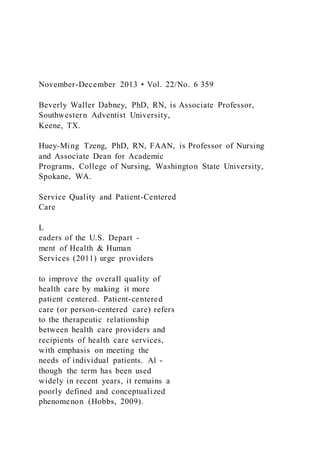
recipients of health care services,
with emphasis on meeting the
needs of individual patients. Al -
though the term has been used
widely in recent years, it remains a
poorly defined and conceptualized
phenomenon (Hobbs, 2009).
Patient-centered care is believed
to be holistic nursing care. It pro-
vides a mechanism for nurses to
engage patients as active partici-
pants in every aspect of their health
(Scott, 2010). Patient shadowing
and care flow mapping were used to
create a sense of empathy and
urgency among clinicians by clarify-
ing the patient and family experi-
ence. These two approaches, which
were meant to promote patient-cen-
tered care, can improve patient sat-
isfaction scores without increasing
costs (DiGioia, Lorenz, Greenhouse,
Bertoty, & Rocks, 2010). A better
under standing of attributes of
patient-centered care and areas for
improvement is needed in order to
develop nursing policies that in -
crease the use of this model in health
care settings.
The purpose of this discussion is
to clarify the concept of patient-cen-
tered care for consistency with the
common understanding about pa -
tient satisfaction and the quality of
care delivered from nurses to
patients. Attributes from a customer
service model, the Gap Model of
Service Quality, are used in a focus
on the perspective of the patient as
the driver and evaluator of service
quality. Relevant literature and the
Gap Model of Service Quality
(Parasuraman, Zeithaml, & Leonard,
1985) are reviewed. Four gaps in
patient-centered care are identified,
with discussion of nursing implica-
tions.
Background and Brief
Literature Review
Patient-Centered Care
The Institute of Medicine (IOM,
2001a) and Epstein and Street (2011)
identified patient-centeredness as
one of the areas for improvement in
health care quality. The IOM (2001b)
defined patient-centeredness as
…health care that establishes a
partnership among practition-
ers, patients, and their families
(when appropriate) to ensure
that decisions respect patients’
wants, needs, and preferences
and that patients have the edu-
cation and support they require
to make decisions and partici-
pate in their own care… (p. 7)
Charmel and Frampton (2008)
defined patient-centered care as
…a healthcare setting in which
patients are encouraged to be
actively involved in their care,
with a physical environment
t ...
November-December 2013 • Vol. 22No. 6 359Beverly Waller D
1. November-December 2013 • Vol. 22/No. 6 359
Beverly Waller Dabney, PhD, RN, is Associate Professor,
Southwestern Adventist University,
Keene, TX.
Huey-Ming Tzeng, PhD, RN, FAAN, is Professor of Nursing
and Associate Dean for Academic
Programs, College of Nursing, Washington State University,
Spokane, WA.
Service Quality and Patient-Centered
Care
L
eaders of the U.S. Depart -
ment of Health & Human
Services (2011) urge providers
to improve the overall quality of
health care by making it more
patient centered. Patient-centered
care (or person-centered care) refers
to the therapeutic relationship
between health care providers and
recipients of health care services,
with emphasis on meeting the
needs of individual patients. Al -
though the term has been used
widely in recent years, it remains a
poorly defined and conceptualized
phenomenon (Hobbs, 2009).
2. Patient-centered care is believed
to be holistic nursing care. It pro-
vides a mechanism for nurses to
engage patients as active partici-
pants in every aspect of their health
(Scott, 2010). Patient shadowing
and care flow mapping were used to
create a sense of empathy and
urgency among clinicians by clarify-
ing the patient and family experi-
ence. These two approaches, which
were meant to promote patient-cen-
tered care, can improve patient sat-
isfaction scores without increasing
costs (DiGioia, Lorenz, Greenhouse,
Bertoty, & Rocks, 2010). A better
under standing of attributes of
patient-centered care and areas for
improvement is needed in order to
develop nursing policies that in -
crease the use of this model in health
care settings.
The purpose of this discussion is
to clarify the concept of patient-cen-
tered care for consistency with the
common understanding about pa -
tient satisfaction and the quality of
care delivered from nurses to
patients. Attributes from a customer
service model, the Gap Model of
Service Quality, are used in a focus
on the perspective of the patient as
the driver and evaluator of service
3. quality. Relevant literature and the
Gap Model of Service Quality
(Parasuraman, Zeithaml, & Leonard,
1985) are reviewed. Four gaps in
patient-centered care are identified,
with discussion of nursing implica-
tions.
Background and Brief
Literature Review
Patient-Centered Care
The Institute of Medicine (IOM,
2001a) and Epstein and Street (2011)
identified patient-centeredness as
one of the areas for improvement in
health care quality. The IOM (2001b)
defined patient-centeredness as
…health care that establishes a
partnership among practition-
ers, patients, and their families
(when appropriate) to ensure
that decisions respect patients’
wants, needs, and preferences
and that patients have the edu-
cation and support they require
to make decisions and partici-
pate in their own care… (p. 7)
Charmel and Frampton (2008)
defined patient-centered care as
…a healthcare setting in which
patients are encouraged to be
4. actively involved in their care,
with a physical environment
that promotes patient comfort
and staff who are dedicated to
meeting the physical, emotion-
al, and spiritual needs of
patients… (p. 80)
In a concept analysis of person-
centered care, Morgan and Yoder
(2011) defined it as
…a holistic (bio-psychosocial-
spiritual) approach to delivering
care that is respectful and indi-
vidualized, allowing negotiation
of care, and offering choice
through a therapeutic relation-
ship where persons are empow-
ered to be involved in health
decisions at whatever level is
desired by that individual who is
receiving the care. (p. 3)
Of significance in various defini-
tions of patient-centered care is the
focus on the patient’s needs, patient
control, and the interaction between
the patient and health care provider.
Being patient-centered suggests
health care providers adapt their
Beverly Waller Dabney
Huey-Ming Tzeng
The Gap Model of Service Quality is used to clarify the concept
5. of
patient-centered care. Four possible patient-centered care
service qual-
ity gaps were identified. Nurse administrators may use these
gaps to
identify and develop appropriate outcome measures.
Instructions for Continuing Nursing Education Contact Hours
appear on page 363.
November-December 2013 • Vol. 22/No. 6360
services to reflect the goals, needs,
and values of the individual patient.
The Joint Commission (2010)
expected hospital leaders to develop
standards to advance effective com-
munication, cultural competence,
and patient- and family-centered
care. Gerteis, Edgman-Levitan, Daley,
and Delbanco (1993) identified
seven dimensions of patient-cen-
tered care needed to improve health
care quality: (a) respect for patients’
values, preferences, and expecta-
tions; (b) coordination and integra-
tion of care; (c) information, com-
munication, and education; (d)
physical comfort; (e) emotional sup-
port and alleviation of fear and anx-
iety; (f) involvement of family and
friends; and (g) transition and conti-
nuity. Communication with pa -
6. tients, which is essential to the appli-
cation of patient-centered care, facil-
itates patient involvement in the
planning of treatment (Hunt, 2009).
Patient-centered care can influ-
ence patient satisfaction, the quality
of health care, and possibly a patient’s
desire to return to a health care
provider for future services (Andrews,
2009; Charmel & Frampton, 2008).
Patients are ex pected to accept more
financial responsibility for their
health care, and they expect value in
their health care purchases as they
would with any other major pur-
chase (Charmel & Frampton, 2008).
McCormack, Manley, and Walsh
(2008) emphasized the significant
role played by health care policy in
developing systems and processes in
health care institutions that are per-
son-centered. The recommendations
of the IOM (2001b) and the Agency
for Healthcare Research and Quality
(2009) to adopt a philosophy of
patient-centeredness have encour-
aged many institutions across the
United States to implement patient-
centered models. A comprehensive
report on patient-centered care was
developed by the Institute for
Family-Centered Care and the
Institute for Health Care Im prove -
ment, from which four key concepts
emerged: (a) respect and dignity, (b)
7. information sharing, (c) participa-
tion, and (d) collaboration (Johnson
et al., 2008). Charmel and Frampton
(2008) indicated the attributes of
patient-centered care need to be clar-
ified to facilitate understanding of
their inter-relatedness. As part of the
promotion of patient-centeredness
for quality improvement, clarifica-
tion of the concept of patient-cen-
tered care is needed (McCormack et
al., 2008).
Communication
The interaction between nurses
and patients is central for the effec-
tive application of patient-centered
care (Hobbs, 2009). Levinson, Lesser,
and Epstein (2010) noted communi-
cation is fundamental to the delivery
of patient-centered care. Nurse-
patient communication seeks to
increase the nurse’s understanding
of the patient’s needs, perspectives,
and values. Nurse-patient communi-
cation also provides patients with
information needed to participate in
their care and assists in correcting
unrealistic expectations. Patient-cen-
tered communication is not simply
agreeing to provide information per
patients’ requests, nor is it throwing
information at patients and leaving
them to sort it out (Epstein, Fiscella,
8. Lesser, & Stange, 2010). Skillful com-
munication with patients helps to
build trust and understanding, and
may require the clinician to engage
in further questioning to explore
fully what the patient hopes to
achieve.
The Joint Commission (2010)
emphasized identification of patient
communication needs as an issue to
be addressed by health care leaders.
Patient communication needs may
include not only language or hearing
barriers, but also emotional or fatigue
barriers. In a qualitative study of
patients with cancer, Montgomery
and Little (2011) found some
patients may be unable or even
unwilling to express their preferences
in regard to treatment during the
debilitating stages of health. They
suggested patients be assessed indi-
vidually for their ability to engage in
such communication; some individ-
uals may need the health profession-
al to assume a greater facilitative role.
The quality of relationships and
interactions between patients and
nurses is of great importance to the
achievement of patient-centered
care. In addition to adequate infor-
mation sharing, structures and
processes are needed to enhance the
delivery of patient-centered care.
9. Delivery of Patient-Centered
Care
Luxford, Safran, and Delbanco
(2011) interviewed senior staff and
patient representatives in a qualita-
tive study. Several organizational
attributes and processes that facili-
tate patient-centered care emerged,
including the following: (a) strong,
committed senior leaders; (b) clear
communication of strategic vision;
(c) active engagement of patients
and families; (d) sustained focus on
staff satisfaction; (e) active measure-
ment and feedback reporting of
patient experiences; (f) adequate
resourcing of care delivery redesign;
(g) staff capacity building; (h)
accountability and incentives; and
(i) a culture supportive of change
and learning. Barriers included the
need to change the organizational
culture from a provider-focus orien-
tation to a patient-focus one, and the
length of time needed for the transi-
tion to take place.
Patient-centered care delivery can
appear superficial and unconvincing
if confusion exists about the mean-
ing of patient-centered care (Epstein
& Street, 2011). Patient-centered
behaviors, such as respecting pa -
tients’ preferences, should be justifi-
10. able on moral grounds alone and
independent of their relationship to
health outcomes. Berwick (2009)
claimed health system design may
affirm patient-centered care as a
dimension of quality in its own
right. Patient-centered care should
not be confirmed just through its
effect on patient or organizational
outcomes. Evidence-base literature
about identifying interventions for
improved outcomes in patient-cen-
tered care is lacking, partially due to
unclear conceptual models and gold-
standard measures (Groene, 2011).
Brief Overview of the Gap
Model of Service Quality
The Gap Model of Service Quality
(Parasuraman et al., 1985) (the Model)
is a widely used business model that
focuses on the perspectives of cus-
November-December 2013 • Vol. 22/No. 6 361
tomers to determine quality and pro-
vides an integrated view of the cus-
tomer-company relationship. The
Model is useful for evaluating
patient-centeredness in nursing care
because of its focus on the customer’s
perspective as a measurement of serv-
ice quality. In addition, it facilitates
11. the derivation of statements of
patient-centered care as an indicator
of quality health care. The Model
included five unique gaps in service
quality that can influence quality as
experienced by the customer. Based
on earlier reports (Charmel &
Frampton, 2008; IOM, 2001a), gaps
number 1, 2, 3, and 5 in the Gap
Model of Service Quality had similar-
ities to the concept of patient-cen-
tered care. A brief description of these
four gaps follows.
Gap 1. Customer expectation vs.
management perception gap. This gap,
also identified as the knowledge gap,
reveals discrepancies between man-
agers’ perceptions of customer
expectations and the actual expecta-
tions of the customers. This gap in
service quality occurs because man-
agers fail to identify customer expec-
tations accurately. The size of the gap
depends on upward communication
from customer to top management
(Parasuraman et al., 1985).
Gap 2. Management perceptions vs.
service standards gap. This gap, also
known as the design gap, measures
how well the managers’ perceptions
of customer expectations are translat-
ed into service design standards.
Service design standards are policies
and expectations of the way service is
12. to be provided. This gap depends on
managers’ belief service quality is
important and possibly dependent
on the resources available for the pro-
vision of the service. However, if
managers’ initial understanding of
customer expectations is flawed, inef-
ficient service standards inevitably
will be produced (Parasuraman et al.,
1985).
Gap 3. Service standards vs. service
delivery gap. This gap, also referred to
as the performance gap, represents
discrepancies between service design
and service delivery. This gap occurs
when the specified policies are not
followed in service delivery. The
quality of delivered service can be
affected by numerous factors, such
as skill level, type of training
received, deficiencies of human
resource policies, failure to match
supply and demand, degree of role
congruity or conflict, and job fit
(Parasuraman et al., 1985).
Gap 5. Perceived service vs. expected
service gap. This is the gap between
customers’ service expectations and
their perceptions of the service
received. According to Parasuraman
and colleagues (1985), customer
expectations are based on word-of-
mouth communications, personal
13. needs, and past experiences.
These four gaps described three
key provider abilities and one cus-
tomer ability: (a) the ability of man-
agers to identify the expectations of
their customers correctly, (b) the abil-
ity to transfer the identified expecta-
tions of their customers into the stan-
dards of service, (c) the ability to
transform these standards of service
into the actual service delivery, and
(d) customers’ perception of how the
delivered service met their expecta-
tions (Parasuraman et al., 1985).
Gaps in Patient-Centered
Care
Based on the Gap Model of
Service Quality (Parasuraman et al.,
1985), four gaps in patient-centered
care were identified (see Figure 1).
Each gap depicted in the model of
patient-centered care quality in nurs-
ing practice is described below.
Gap A. Patient expectation vs. nurse
perception gap was derived from Gap
1 in the Gap Model of Service
Quality. This gap occurs when dis-
crepancies arise between nurses’ and
nursing administrators’ perceptions
of what the patient expects and the
patient’s actual expectations. The
health care provider fails to identify
14. the patient’s expectations accurately.
Lack of communication with the
patient and an insufficient relation-
ship focus are key contributors to
this gap.
To close this gap, nurses must com-
municate with the patient in a way
that gathers his or her expectations
and needs. Epstein and co-authors
(2010) noted the communication
goes beyond facts and figures. The cli-
nician must frame and tailor informa-
tion in response to an understanding
of the patient’s concerns, beliefs, and
experiences. Aspects of the patient’s
culture, past experiences, his or her
perceptions from comments made by
others, and immediate personal
needs all shape what the patient
desires and expects from health care
services. The key to closing this gap is
to reach consensus about an
approach to care which is achieved
through shared deliberation.
Gap B. Nurse and nursing adminis-
trator perceptions vs. patient-centered
care standards gap was derived from
Gap 2 in the Gap Model of Service
Quality. This gap depends on the
health care provider’s and adminis-
trator’s beliefs that patient-centered
care is important to quality of care
and it is possible to provide patient-
15. centered care. This gap is measured
by how well the health care delivery
design matches the health care
provider’s perceptions of the pa -
tient’s expectations or needs. Indi -
vidual nurses have their own sets of
values and service standards based
on their backgrounds and what they
perceive the patient’s expectations to
be. This gap is measured by how well
the health care delivery design
matches the health care provider’s
perceptions of the patient’s expecta-
tions or needs.
To close this gap, nurse administra-
tors must decide that meeting the
needs of individual patients is a prior-
ity, set organizational standards, and
provide resources necessary to meet
those standards. Individual nurses
must decide if the provision of
patient-centered care is a priority. The
infrastructure of patient-centered care
is supported through the senior nurs-
ing team’s commitment to the princi-
ples of patient-centered care. How -
ever, development of appropriate
standards is contingent on identify-
ing patient needs correctly.
Gap C. Patient-centered care stan-
dards vs. delivery of patient-centered
care gap was derived from Gap 3 in
the Gap Model of Service Quality.
This gap represents variations in
16. service design and service delivery.
The service standards are to be
derived from the perceived expecta-
tions of patients. Service standards
are based on the principles of
Service Quality and Patient-Centered Care
November-December 2013 • Vol. 22/No. 6362
patient-centered care, and need to be
translated to actual delivery of care.
Nurses can have great impact on
closing this gap.
In practice, patient-centered care
is not offered consistently due to
nursing factors, such as poor staffing,
fatigue, burnout, and lack of educa-
tion on the delivery of patient-cen-
tered care. A qualitative meta-syn-
thesis of four studies found evidence
of sustained high commitment nec-
essary to the development of person-
centered cultures in clinical settings
(McCormack, Karlsson, Dewing, &
Lerdal, 2010). However, other cultur-
al characteristics (e.g., the level of
staff support) may determine the
extent to which that commitment
could be sustained.
Gap D. Patient expectation of health
17. care service vs. patient perception of
actual health care service received gap
was derived from Gap 4 in the Gap
Model of Service Quality. This gap
occurs when the patient’s expecta-
tions, which are molded by past
experiences, culture, personal needs,
and word of mouth, are not met or
are lacking in some way (Hunt,
2009; Parasuraman et al., 1985). In
other words, when care is not
patient-centered, patient expecta-
tions cannot be met because they are
not identified. McCormack and co-
authors (2008) suggested a direct
relationship between patients’ expe-
riences of daily care and their percep-
tions of service effectiveness.
To close this gap and understand
patient preferences, nursing adminis-
trators need to promote an interac-
tive feedback loop that provides
health care providers with a mecha-
nism to view care through the eyes of
patients and families as well as to link
the patients and nursing staff togeth-
er (DiGioia et al., 2010). A collabora-
tive relationship between health care
providers and patients can assist in
shaping realistic patient expectations
FIGURE 1.
The Four-Gap Model of Patient-Centered Care Quality in
Nursing Practice
18. Quality of
Patient-Centered
Care in Nursing
Practice
Patient perceived
service
Patient
expectation
Delivery of
patient-centered
standards
Nurse and
nursing
administrator
perception of patient
expectation
Nurse and nursing
administrator transla-
tion of perceptions into
patient-centered care
standards
19. Gap B:
Nurse and nursing
administrator perceptions
vs. patient-centered care
standards gap
Gap D: Patient expectation of
health care service vs. patient
perception of actual health care
service received gap
Gap A:
Patient expectation
vs. nurse
perception gap
Gap C:
Patient-centered care
standards vs.
delivery of patient-
centered care gap
November-December 2013 • Vol. 22/No. 6 363
related to patients’ individual health
care needs, and minimize false per-
ceptions due to lack of understand-
ing. A complex series of interactions
between nurses and patients elicit
20. trust and understanding. Nurses
need to use the knowledge gathered
from these interactions to adapt a
plan of care that reflects individual
patient needs.
Nursing Implications
Nurses may use the four-gap
model of patient-centered care qual-
ity (see Figure 1) to examine their
practice. This approach will provide
opportunity to identify gaps as well
as develop nursing practice interven-
tions to close the gaps indicated in
this new model. For example, nurse
executives and managers may devel-
op appropriate outcome measures to
monitor the closeness of each corre-
sponding gap (e.g., patient satisfac-
tion measures; patient-centered out-
comes such as survival, function,
symptoms, and health-related quali-
ty of life; clinical outcomes such as
injurious fall occurrences, nurses’ job
satisfaction measures, and intention
to quit) (DiGioia et al., 2010, Patient-
Centered Outcomes Research, 2013).
Future Research
The four-gap model of patient-cen-
tered care quality in nursing practice
needs to be tested. Understanding the
nurse-patient relationship and the
aspects of communication needed for
21. successful outcomes is essential. A
focus on patient perspectives assists in
capturing cultural, spiritual, and emo-
tional needs that otherwise may be
missed or overlooked. Future research
that captures the degrees of similarity
or difference between patient per-
spectives and provider perspectives
will help identify areas of strengths
and weaknesses for improvement.
Future research also may explore the
links between system issues, such as
the effects of nurse staffing on the
ability to deliver patient-centered
care, and the developmental process
of standards and policy for delivery of
patient-centered care.
Conclusion
Four patient-centered care serv-
ice quality gaps were identified.
Individual patient needs influence
expectations, and accurate nurse
perceptions of these needs require
communication with the patient.
Collaboration between nurses and
patients is essential to provide bet-
ter understanding of patient needs
and helps patients understand
what to expect realistically from
their health care experience. Once
pa tient needs have been assessed
accurately and understood, poli-
cies relevant to the characteristics
of the clinical settings can be estab-
22. lished to promote patient-centered
care. McClelland (2010) claimed
understanding the patient perspec-
tive of health care services is piv-
otal to the development of patient-
centered, quality services. The shift
of health care from a clinician-cen-
tric orientation to a patient-centric
one can be challenging to the
entire health care team. However,
to realize fully the benefits of
patient-centered care, nurses must
focus on achieving gains in the
quality of relationships and inter-
actions with patients (Epstein et
al., 2010).
REFERENCES
Agency for Healthcare Research and Quality.
(2009). National healthcare quality
report. Retrieved from http://ahrq.gov/
qual/qrdr09.htm
Andrews, S.M. (2009). Patient family-centered
care in ambulatory surgery setting.
Journal of PeriAnesthesia Nursing,
24(4), 244-246. doi:10.1016/j.jopan.
2009.05.100
Berwick, D. (2009). What ‘patient-centered’
should mean: Confessions of an extrem-
ist. Health Affairs, 28(4), w555-w565.
Charmel, P.A., & Frampton, S.B. (2008).
Building the business case for patient-
23. centered care. Healthcare Financial
Management, 62(3), 80-85.
DiGioia, A., III, Lorenz, H., Greenhouse, P.K.,
Bertoty, D.A., & Rocks, S.D. (2010). A
patient-centered model to improve met-
rics without cost increase: Viewing all
care through the eyes of patients and
families. Journal of Nursing Admini -
stration, 40(12), 540-546.
Epstein, R.M., & Street, R.L. (2011). The val-
ues and value of patient-centered care.
Annals of Family Medicine, 9(2), 100-
103.
Epstein, R., Fiscella, L., Lesser, C., & Stange,
K. (2010). Why the nation needs a policy
push on patient-centered health care.
Health Affairs, 29(8), 1489-1495.
Gerteis, M., Edgman-Levitan, S., Daley, J., &
Delbanco, T.L. (1993). Introduction:
Service Quality and Patient-Centered Care
Instructions For
Continuing Nursing
Education Contact Hours
Service Quality and Patient-
Centered Care
Deadline for Submission:
December 31, 2015
24. MSN J1322
To Obtain CNE Contact Hours
1. For those wishing to obtain CNE con-
tact hours, you must read the article
and complete the evaluation through
AMSN’s Online Library. Complete
your evaluation online and print your
CNE certificate immediately, or later.
Simply go to www.amsn.org/library
2. Evaluations must be completed online
by December 31, 2015. Upon comple-
tion of the evaluation, a certificate for 1.3
contact hour(s) may be printed.
Fees – Member: FREE Regular: $20
Objectives
This continuing nursing educational (CNE)
activity is designed for nurses and other
health care professionals who are interest-
ed in service quality and patient-centered
care. After studying the information pre-
sented in this article, the nurse will be able
to:
1. Describe patient-centered care.
2. Discuss gaps in patient-centered care.
3. Explain the nursing implications of using
the Gap Model of Service Quality to clar-
ify patient-centered care.
Note: The authors, editor, and education
25. direc tor reported no actual or potential
conflict of interest in relation to this continuing
nursing education article.
This educational activity has been co-provided
by AMSN and Anthony J. Jannetti, Inc.
Anthony J. Jannetti, Inc. is a provider
approved by the California Board of Registered
Nursing, provider number CEP 5387. Licensees
in the state of CA must retain this certificate for
four years after the CNE activity is completed.
Anthony J. Jannetti, Inc. is accredited as a
provider of continuing nursing education by the
American Nurses’ Credentialing Center’s
Commission on Accreditation.
This article was reviewed and formatted for
contact hour credit by Rosemarie Marmion,
MSN, RN-BC, NE-BC, AMSN Education
Director. Accreditation status does not imply
endorsement by the provider or ANCC of any
commercial product.
November-December 2013 • Vol. 22/No. 6364
Medicine and health from the patient’s
perspective. In M. Gerteis, S. Edgman-
Levitan, J. Daley, & T.L. Delbanco (Eds.),
Through the patient’s eyes: Under -
standing and promoting patient-centered
care (pp. 1-15). San Francisco, CA:
Jossey-Bass.
26. Groene, O. (2011). Patient centeredness and
quality improvement efforts in hospitals:
Rationale, measurement, implementa-
tion. International Journal for Quality in
Health Care, 23(5), 531-537.
Hobbs, J.L. (2009). A dimensional analysis of
patient-centered care. Nursing Re -
search, 58(1), 52-62.
Hunt, M.R. (2009). Patient-centered care and
cultural practices: Process and criteria
for evaluating adaptations of norms and
standards in health care institutions.
HEC Forum, 21(4), 327-339.
Institute of Medicine (IOM). (2001a). Six aims
for improvement. In Crossing the quality
chasm (pp. 41-61). Washington, DC:
National Academy Press.
Institute of Medicine (IOM). (2001b).
Executive summary. In M.P. Hurtado,
E.K. Swift, & J.M. Corrigan (Eds.),
Envisioning the national healthcare qual-
ity report (pp. 1-18). Washington, DC:
National Academy Press. Retrieved from
http://books.nap.edu/catalog.php?
record_id=10073
Johnson, B., Abraham, M., Conway, J.,
Simmons, L., Edgman-Levitan, S.,
Sodomka, P., … Ford, D. (2008).
Partnering with patients and families to
design a patient and family centered
27. healthcare system. Bethesda, MD:
Institute of Family Centered Care.
Levinson, W., Lesser, C.S., & Epstein, R.M.
(2010). Developing physician communi-
cation skills for patient-centered care.
Health Affairs, 29(7), 1310-1318.
Luxford, K., Safran, D.G., & Delbanco, T.
(2011). Promoting patient-centered care:
A qualitative study of facilitators and bar-
riers in healthcare organizations with a
reputation for improving the patient expe-
rience. International Journal for Quality in
Health Care, 23(5), 510-515.
McClelland, H. (2010). Service improvement
and patient experience. International
Emergency Nursing, 18(4), 175-176.
McCormack, B., Karlsson, B., Dewing, J., &
Lerdal, A. (2010). Exploring person-cen-
teredness: A qualitative meta-synthesis
of four studies. Scandinavian Journal of
Caring Sciences, 24(3), 620-634.
McCormack, B., Manley, K., & Walsh, L.
(2008). Person-centered systems and
processes. In K. Manley, B. McCormack,
& V. Wilson V (Eds), International prac-
tice development in nursing and health-
care (pp. 17-41). Oxford, England:
Blackwell Publishing.
Montgomery, K., & Little, M. (2011). Enriching
patient-centered care in serious illness: A
28. focus on patients’ experiences of
agency. The Milbank Quarterly, 89(3),
381-398.
Morgan, S.S., & Yoder, L. (2011). A concept
analysis of person-centered care. Jour -
nal of Holistic Nursing. doi:10.1177/
0898010111412189
Parasuraman, A., Zeithaml, V., & Leonard, B.
(1985). A conceptual model of service
quality and its implications for further
research. Journal of Marketing, 49(4),
41-50.
Patient-Centered Outcomes Research.
(2013). Patient-centered outcomes re -
search. Retrieved from http://www.pcori.
org/research-we-support/pcor/
Scott, A. (2010). Quality lessons. Patient-
centered care vital to outcomes, cost.
Modern Healthcare, 40(46), 22.
The Joint Commission. (2010). Advancing
effective communication, cultural compe-
tence, and patient- and family-centered
care: A roadmap for hospitals. Oakbrook
Terrace, IL: Author.
U.S. Department of Health & Human Services.
(2011). National quality strategy will pro-
mote better health, quality care for
Americans (press release). Retrieved
from http://www.hhs.gov/news/press/
2011pres/03/20110321a.html
29. Copyright of MEDSURG Nursing is the property of Jannetti
Publications, Inc. and its content
may not be copied or emailed to multiple sites or posted to a
listserv without …