This document provides an overview of glomerular causes of hematuria including definitions, diagnostic workup, differential diagnoses, and treatment approaches. Key points discussed include:
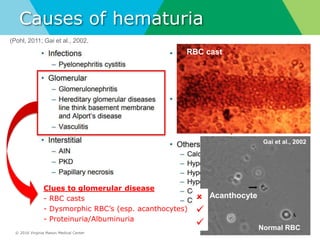
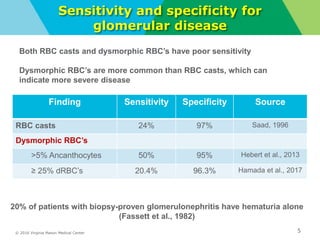
- Definitions of gross and microscopic hematuria and their clinical significance. Dysmorphic red blood cells and red blood cell casts can indicate glomerular disease but have low sensitivity.
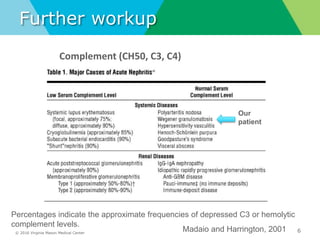
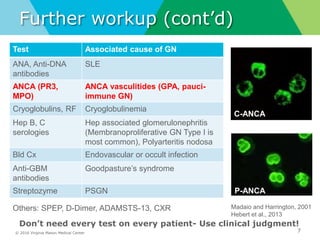
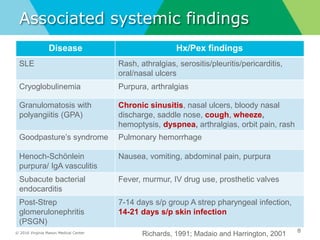
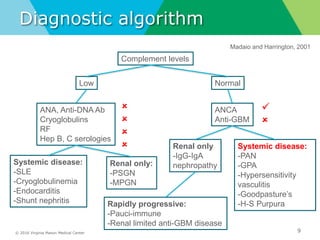
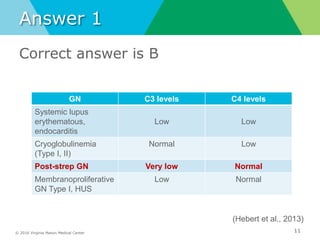
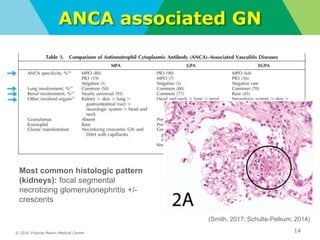
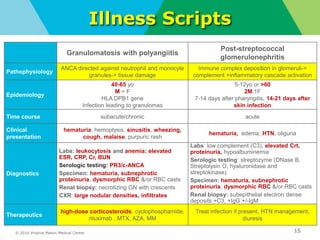
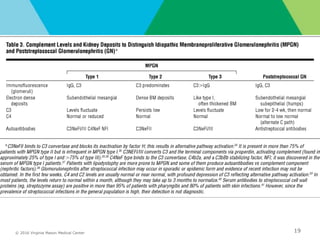
- Diagnostic workup may include complement levels, ANCA, ANA, hepatitis and cryoglobulin serologies to identify underlying causes like ANCA-associated glomerulonephritis, lupus, or hepatitis.
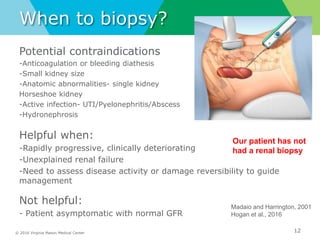
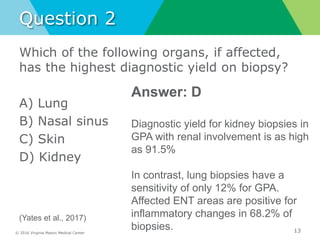
- Biopsy of the kidney has the highest diagnostic yield compared to other organs and should be considered for rapidly progressive or unexplained



























































![2019 04-30 noon conference [stephen slade]](https://cdn.slidesharecdn.com/ss_thumbnails/2019-04-30noonconferencestephenslade-190501212611-thumbnail.jpg?width=640&height=640&fit=bounds)





























