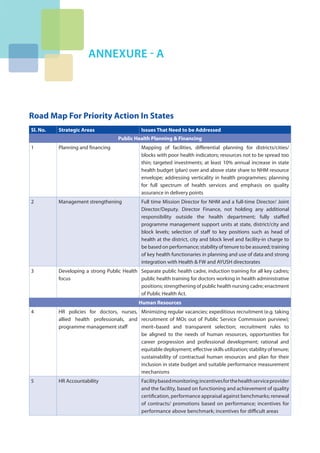
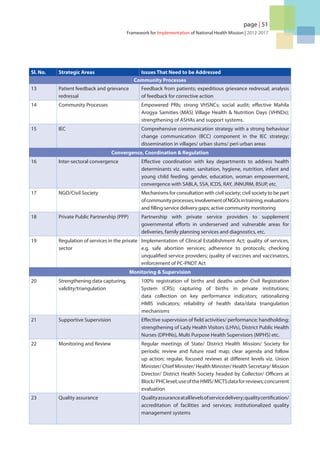
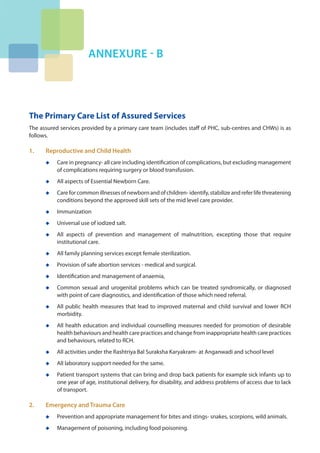
This document provides the framework for implementation of India's National Health Mission from 2012-2017. It lays out the vision, guiding principles, and core values of the NHM, which include attaining universal access to equitable, affordable, and quality healthcare. The key goals are to enable achievement of the vision, make the system responsive to citizen needs, build partnerships to realize health goals, focus on survival and well-being of women and children, reduce disease burden, and ensure financial protection for households. The strategies to achieve these goals include supporting state health system strengthening, building state and district capacity for decentralized outcome-based planning, enabling integrated facility development, and creating district knowledge centers.