College of Education
Schoolof Continuing and Distance Education
2014/2015 – 2016/2017
NURS 233
Medical Microbiology and Parasitology
Session 8 – Mycobacterial Infections –
Tuberculosis (Tb)
Lecturer: Prof. Kwasi Addo, SON, UG
Contact Information: kaddo@noguchi.ug.edu.gh
2.
Session Overview
• Tuberculosiscontinues to be a major public health
problem worldwide. This session seeks to discuss the
genus mycobacterium with particular attention on
tuberculosis.
Goals and Objectives
• At the end of the session, the student will:
• Understand the genus mycobacterium
• Describe the general properties of mycobacterium
• Describe the mycobacterial cell wall
• Illustrate the Global TB situation
Prof. Kwasi Addo, SON, UG Slide 2
3.
Goals and ObjectivesCont’d
• List the causative agents of TB
• Describe the types of TB
• Identify the modes of TB Transmission
• Describe the pathogenesis of TB
• Explain the Laboratory diagnosis of TB
• Describe the treatment regimens
• Explain drug resistance TB
• Discuss the Control and Prevention of TB
Prof. Kwasi Addo, SON, UG Slide 3
4.
Session Outline
The keytopics to be covered in the session are as follows:
• Mycobacterial Diseases
• Tuberculosis (Tb)
• Pathophysiology
• Laboratory Diagnosis
• Multi and Extensively Drug Resistance TB
• Treatment
Prof. Kwasi Addo, SON, UG Slide 4
5.
Reading List
• Chapter56 of Recommended Text – Cook G. C. and
Zumla, A. (2005). Manson’s Tropical Diseases
Prof. Kwasi Addo, SON, UG Slide 5
THE ORGANISM
• Mycobacteriacaused disease in humans and animals
long before recorded history with evidence of disease
found in the bones of prehistoric humans and animals
• Mycobacterium is currently the only genus in the
Mycobacteriaceae family, although there has been
proposals to include Corynebacterium, Nocardia and
Rhodococcus in this family
• There are over 200 species of mycobacteria. Majority
are harmless and found abundantly in the environment
Prof. Kwasi Addo, SON, UG Slide 7
8.
GENERAL PROPERTIES
• Mycobacteriashared general properties that distinguish it from
other related species. They are:
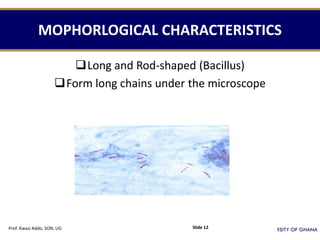
1. Straight or slightly curved rod-shaped organisms
2. Small or thin in size
3. Size of 0.2 - 0.6 x 1.0 - 10 µm
4. Cells are Gram-positive though not easily stainable by Gram-stain
method
5. Stained by Ziehl-Neelsen method
6. Acid-fast organisms
7. Non-sporing, non-motile
8. Aerobic or microaerophilic
9. Grown on egg based culture medium
10. Waxy lipid cell wall (over 60% of the dry cell weight, compared with 3%
in Gram-negative bacteria and 0.5% in Gram-positive spp.)
11. The high lipid content gives the mycobacteria a high level of resistance to
drying, alcohol, acids, alkali, many disinfectants and most antibiotics
Prof. Kwasi Addo, SON, UG Slide 8
9.
MYCOBACTERIAL CELL WALL
•Mycobacteria have the most complex of all known cell walls
• Stripped of its unique cell wall, mycobacteria is just like any
other bacteria
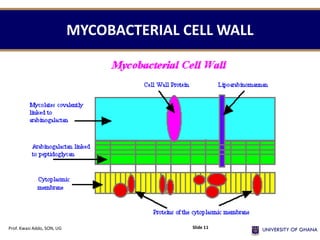
• This unique cell wall consist of 4 main layers overlying the cell
membrane
• The innermost layer is called Murein or Peptidoglycan and this
gives the cell its shape and rigidity and also the powerful
adjuvant activity of mycobacteria
• The 2nd layer is called Arabinogalactan layer which is a
branched macromolecule consisting of arabinose and galactose
Prof. Kwasi Addo, SON, UG Slide 9
10.
MYCOBACTERIAL CELL WALL
•The side chains of the arabinogalactan are linked to the 3rd
layer, consisting of Mycolic acids which are long-chain
fatty acids 60-90 carbon atoms
• Mycolic acid is a major component of the mycobacterial
cell wall and contributes to its thickness and to a larger
extent for the acid-fastness character of mycobacteria
• The 4th or outer layer – Mycoside is very thick and gives
colonies a very smooth appearance. It consist of high lipid
and related compounds such as phenolic glycosides,
glycolipids, peptidoglycolipids and Wax D.
Prof. Kwasi Addo, SON, UG Slide 10
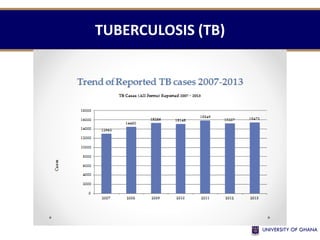
TUBERCULOSIS (TB)
• TBis a communicable disease caused by the
Mycobacterium tuberculosis complex
• Members of the complex are:
1. M. tuberculosis 6. M. canetti
2. M. bovis 7. M. pinnipedii
3. M. africanum
4. M. microti
5. M. bovis-BCG
• The 7 species are closely related genetically and differ
only in their epidemiology
Prof. Kwasi Addo, SON, UG Slide 17
18.
M. TUBERCULOSIS COMPLEX
•M. tuberculosis causes TB in humans and animals that
have contact with humans
• M. bovis causes bovine TB in cattle, sheep, goats, and
other domestic and wild animals and also in man
• M. africanum is an intermediate species between M.
tuberculosis and M. bovis. It causes TB in man, primates,
pigs and cattle
• M. microti causes TB in voles (Microtus agrestis) and other
small rodents such as hamsters, rats, mice, rabbits and
guinea pigs, but attenuated in humans
Prof. Kwasi Addo, SON, UG Slide 18
19.
M. TUBERCULOSIS COMPLEX
•M. bovis BCG is termed the vaccine strain and can
cause disseminated BCG infection in vaccinated
children
• M. canetti is rarely seen but can cause TB in humans
• M. pinnipedii is described as the seal bacillus for
causing TB in fish-eating sea animals
Prof. Kwasi Addo, SON, UG Slide 19
PULMONARY TUBERCULOSIS (PTB)
•It is a type of TB affecting mainly the lungs’
parenchymal tissue
• Tubercle bacilli multiplies well in an environment
with high oxygen tension, hence predominant
infection is mostly pulmonary
• PTB is the most common form of the disease,
occurring in over 80% of all TB cases.
• It is the only form of TB which is highly infectious.
Prof. Kwasi Addo, SON, UG Slide 21
22.
CLINICAL SYMPTOMS OFPTB
• Persistent cough for 2 weeks or more
• Sputum production which may be blood-stained
(haemoptysis)
• Chest pain
• Shortness of breath
• Fatigue
• Fever
• Night sweats
• Weight loss
• Poor appetite
• General feeling of illness (malaise)
Prof. Kwasi Addo, SON, UG Slide 22
23.
EXTRAPULMONARY TUBERCULOSIS
(EPTB)
• Itis TB affecting any organ other than the lungs’
parenchymal tissue
• It can involve organs such as lymph nodes, spine,
bones and joints, the urogenital tract, the nervous
system, the intestine and many other parts of the body
• EPTB cases are almost never infectious unless they
have PTB as well
• Symptoms of the disease depend on the organ
involved
Prof. Kwasi Addo, SON, UG Slide 23
24.
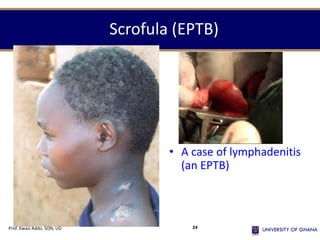
Scrofula (EPTB)
• Acase of lymphadenitis
(an EPTB)
Prof. Kwasi Addo, SON, UG 24
25.
RISK FACTORS FORINFECTION
• Exposure to TB bacilli
• Duration of exposure to a person with PTB
• Intensity of exposure
• Untreated AFB smear positive PTB
• Cases are the most infectious
Prof. Kwasi Addo, SON, UG Slide 25
26.
RISK FACTORS FORDISEASE
• Development of disease depends on individual
susceptibility
• HIV increases the risk of getting TB disease
• 10% Life time risk of TB in HIV negative
• 10% Annual risk of TB in HIV positive
Prof. Kwasi Addo, SON, UG Slide 26
27.
MODE OF TRANSMISSION
•It is mainly through aerosol or inhalation of the
bacilli
• Coughing, sneezing, spitting, speaking and singing
by an infectious person expels bacilli into the air
in tiny droplets and transmission commonly occur
by inhalation of these aerosols
• Ingestion through alimentary or digestive route of
contaminated meat or fresh unpasteurized milk
may lead to intestinal TB
Prof. Kwasi Addo, SON, UG Slide 27
How is TBspread ?
• Coughs
• Sneezes
• Shouts
• Sings
• Talks
TB germs can be spread when a person with TB disease:
sending TB germs into the air
Prof. Kwasi Addo, SON, UG 29
30.
You get TB
frombeing in
VERY CLOSE
CONTACT with
someone who
is sick with TB
disease.
Prof. Kwasi Addo, SON, UG 30
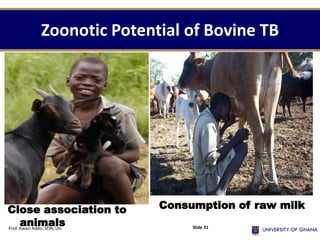
31.
Zoonotic Potential ofBovine TB
Prof. Kwasi Addo, SON, UG Slide 31
Close association to
animals
Consumption of raw milk
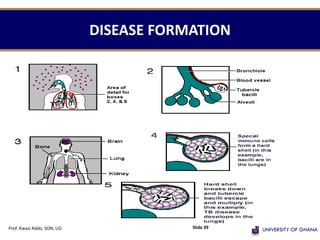
PATHOGENESIS 1
• Whenmoist droplets of saliva or mucous containing tubercle
bacilli are produce by an infectious person, these droplets
travel far and get suspended in the air for several hours
• These aerosols of infective particles may be inhaled by
another person
• If the bacilli establish themselves in the lungs of the person
and begin to multiply, then primary infection has occurred
• Among those who become infected nearly 90% never
manifest the disease and the bacilli remain dormant within
the body
• Only in small numbers – 10% does the primary infection
develops into progressive disease
Prof. Kwasi Addo, SON, UG Slide 36
37.
PATHOGENESIS 2
• Ingestionof the bacilli by phagocytes turns them into
phagosomes and this gives protection to the bacilli from
bactericidal components of serum.
• Later, lysosomes fuse themselves to the phagosomes to
form phagolysosomes and it is here that phagocytes
attempt to kill unsuccessfully the bacilli by releasing into
the phagosomes hydrolytic enzymes.
• The bacilli after escaping death, then multiply and destroy
the phagocytes.
• Other phagocytes enters the area and ingest the increasing
numbers of tubercle bacilli and a small cluster of cells
known as granuloma develops.
Prof. Kwasi Addo, SON, UG Slide 37
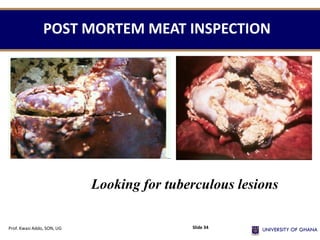
38.
PATHOGENESIS 3
• Cellularresponses attempting to control the
disease result in the accumulation of large
numbers of phagocytes and finally macroscopic
lesions called tubercle is formed.
• The tubercle is a characteristic lesion of TB.
Initially it is grey, transparent nodule but as the
lesion develops, caseous degeneration starts in
the centre to give the tubercle a yellowish cast.
Prof. Kwasi Addo, SON, UG Slide 38
LABORATORY DIAGNOSIS
• Thisis to support clinical diagnosis
MICROSCOPY
The Ziehl-Nelseen staining technique
• For diagnosis 2 sputum specimen are requested
on spot
early morning
• For follow-up (2(3),5,6 months of treatment) 1 specimen is
requested.
• For AFB to be detected microscopically, there must be
between 5,000 and 10,000 bacilli in 1 ml of sputum.
Prof. Kwasi Addo, SON, UG Slide 41
42.
NEW POLICY
• “Consistentwith WHO recommendations, the
NTP has made a policy decision that from 2010,
the number of sputum specimens to be examined
for screening of TB suspects be reduced from
three to two.
• This change from three to two sputum strategy
has been made based on concrete evidence that
has shown that the first and second sputum
samples pick as higher as 97% of TB cases.
Prof. Kwasi Addo, SON, UG Slide 42
43.
NEW POLICY 2
•Furthermore, this two sputa strategy will reduce the
laboratory workload.
• These sputum samples will be collected as one “spot” and
one “morning.”
• In a situation where the patient comes far away from the
sputum smear microscopy centre second sputum sample
can be collected one hour after the first “spot” sample
using a novel strategy which is now referred to as “Front-
loaded” or “Same Day” or “one Stop shop” microscopy.
• In order to successfully implement these innovative
strategies external quality assurance (EQA) for smear
microscopy has to be well functioning”.
Prof. Kwasi Addo, SON, UG Slide 43
44.
Never Stand inFront of the Patient During
Collection
Prof. Kwasi Addo, SON, UG Slide 44
45.
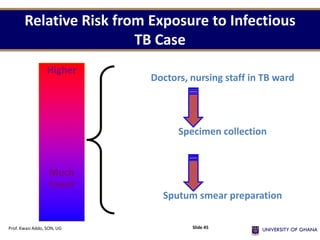
Relative Risk fromExposure to Infectious
TB Case
Higher
Much
lower
Doctors, nursing staff in TB ward
Specimen collection
Sputum smear preparation
Prof. Kwasi Addo, SON, UG Slide 45
46.
Personnel Protective Equipment:Masks
• Surgical masks do not
filter out infectious
droplet nuclei
• N95 respirators are
most appropriate
Prof. Kwasi Addo, SON, UG 46
47.
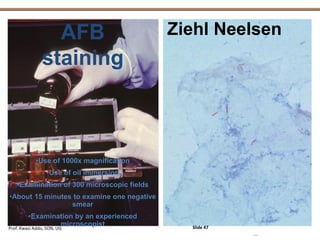
AFB
staining
Ziehl Neelsen
•Use of1000x magnification
•Use of oil immersion
•Examination of 300 microscopic fields
•About 15 minutes to examine one negative
smear
•Examination by an experienced
microscopist
Prof. Kwasi Addo, SON, UG Slide 47
ADVANTAGES OF AFBSMEAR MICROSCOPY
• Microscopy is a simple convenient test
• Requires minimal infrastructure and equipment
• Highly accurate, inexpensive and fast
• Accessible to the majority of patients
• Prioritizes infectious cases
Prof. Kwasi Addo, SON, UG Slide 51
52.
LIMITATIONS OF MICROSCOPY
•Can not distinguish between dead or live bacteria
• High bacterial load >3000–5000 AFB /mL is
required for detection
• Can not do species identification
• Can not perform DST
Prof. Kwasi Addo, SON, UG Slide 52
53.
"New policies“ ReducingDiagnostic Delay
• Liquid culture and DST and rapid
speciation
• Line-probe assay for detecting
resistance to rifampicin and isoniazid
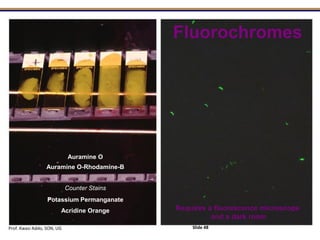
• LED fluorescent microscopy
• Smear-positive case definition based
on a patient having one positive
sputum smear (≥ 1 AFB per smear)
instead of two positive smears
• Gene Xpert
Prof. Kwasi Addo, SON, UG Slide 53
54.
"New policies"
• Algorithmfor the diagnosis of TB in HIV-positive
people, which includes use of all investigations at
the same time including CXR, culture (when
available) and no use of an antibiotic trial
• Use of 6 month regimen
• Use of FDCs
• PPM DOTS expansion
• Use of ISTC
• TB screening in HIV +
• Contact investigation
Prof. Kwasi Addo, SON, UG Slide 54
55.
LABORATORY DIAGNOSIS 2
•CULTURE
Egg based media such as Lowenstein-Jensen and
Ogawa are used
The media contains egg, glycerol, asparagine, mineral
salts and malachite green dye
It takes 4-8 weeks of incubation at 37ºC to see visible
colonies of mycobacteria
• SENSITIVITY
The proportion method is used
• MOLECULAR TECHNIQUES
Polymerase Chain Reaction (PCR), DNA Fingerprinting
Prof. Kwasi Addo, SON, UG Slide 55
56.
TB CULTURE –L-J MEDIA
Prof. Kwasi Addo, SON, UG Slide 56
57.
DRUG SUSCEPTIBILITY TESTING
Paramountfor
treatment failures,
relapses and chronic
excreters
Helps to define DR,
MDR & XDR-TB
Prof. Kwasi Addo, SON, UG Slide 57
58.
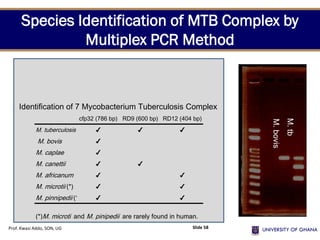
cfp32 (786 bp)RD9 (600 bp) RD12 (404 bp)
M. tuberculosis ✔ ✔ ✔
M. bovis ✔
M. caplae ✔
M. canettii ✔ ✔
M. africanum ✔ ✔
M. microtii (*) ✔ ✔
M. pinnipedii (*) ✔ ✔
(*)M. microti and M. pinipedii are rarely found in human.
Identification of 7 Mycobacterium Tuberculosis Complex
M.
bovis
M.
tb
Species Identification of MTB Complex by
Multiplex PCR Method
Prof. Kwasi Addo, SON, UG Slide 58
MYCOBACTERIA GROWTH INDICATORTUBE (MGIT)
• MGIT tubes are round-bottom glass tubes, each containing
4ml of modified Middlebrook 7H9 broth at pH 6.7 and
flushed with 10% CO2.
• On the tube bottom is fluorescent indicator embedded in a
silicon base.
• For rapid growth of mycobacteria, the broth is supplemented
with OADC and PANTA.
• OADC (Oleic acid, albumin, dextrose and catalase) is for
growth enhancement.
• PANTA (Polymycin, amphotericin, nalidixic acid,
trimethoprim and azlocilin) is a mixture of antibiotics and is
used for reducing contamination.
Prof. Kwasi Addo, SON, UG Slide 60
61.
GENERAL PRINCIPLE
• Thefluorescent compound at the bottom of the tube is
sensitive to the presence of oxygen dissolved in the broth
• The large amount of dissolved oxygen quenches the
emission from the compound and little fluorescence can be
detected
• After adding OADC and PANTA the broth is inoculated with
the pre-treated specimen
• Actively respiring mycobacteria consume the oxygen and
allow the fluorescence to be observe at the bottom and
meniscus
• GROWTH IS BETWEEN 4-6 DAYS
• No growth is declared after 6 weeks
Prof. Kwasi Addo, SON, UG Slide 61
62.
LIMITATIONS OF CULTURE
•Greater need for
– infrastructure, qualified staff, equipment, and additional
safety measures
• Increased time: weeks for result
• More sensitive to technical deficiencies
• Expensive
Prof. Kwasi Addo, SON, UG Slide 62
63.
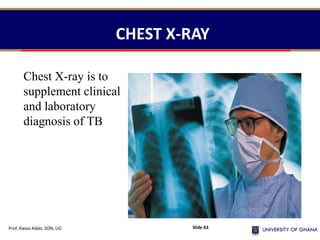
CHEST X-RAY
Chest X-rayis to
supplement clinical
and laboratory
diagnosis of TB
Prof. Kwasi Addo, SON, UG Slide 63
• The WHOstrongly recommend that
commercial serodiagnostic tests not
be used for the diagnosis of
pulmonary and extra-pulmonary TB.
• Currently available commercial
serodiagnostic tests (also referred to
as serological tests) provide
inconsistent and imprecise findings.
• There is no evidence that existing
commercial serological assays improve
patient outcomes, and high
proportions of false-positive and
false-negative results may have an
adverse impact on the health of
patients.
COMMERCIAL SERODIAGNOSTIC TESTS FOR DIAGNOSIS OF
ACTIVE TUBERCULOSIS
Prof. Kwasi Addo, SON, UG Slide 65
66.
• It consistsof an instrument, personal computer, barcode
scanner, and preloaded software, and uses single-use
disposable cartridges containing lyophilized reagents, buffers
and washes.
• Target detection and characterization is performed in real
time using a six-color laser detection device.
• Developed in 2009 and endorsed by WHO in Dec 2010, it is
considered an important breakthrough in the fight against TB.
• For the first time, a molecular test is simple and robust
enough to be introduced outside conventional laboratory
settings.
• It detects M. tuberculosis as well as rifampicin resistance
directly from sputum within 100 minutes.
GENEXPERT SYSTEM
Prof. Kwasi Addo, SON, UG Slide 66
67.
GenXpert MTB/RIF SYSTEM
Automatedreal-time
nucleic acid
amplification
technology for rapid
and simultaneous
detection of TB and
rifampicin resistance
Prof. Kwasi Addo, SON, UG Slide 67
68.
• Xpert MTB/RIFis suitable for use at district and sub-district
level (at point of care)
• Adoption of Xpert MTB/RIF does not eliminate the need for
conventional TB microscopy, culture and DST capacity.
Microscopy and/or culture remains necessary for monitoring
of treatment, as it is unlikely that a test based on DNA
detection would be suitable
• Xpert MTB/RIF should therefore not be used for monitoring
of treatment. In addition, conventional culture and DST are
still required to detect resistance to anti-TB drugs other than
rifampicin.
SITING OF THE Xpert
Prof. Kwasi Addo, SON, UG Slide 68
69.
• Cost-comparisons showthat the current running costs of
Xpert MTB/RIF (16.86 USD per test) are substantially greater
than those of microscopy, but less than the cost for
performing culture and DST (around 20 USD per test using
solid culture and around 30 USD per test using liquid culture).
• Initial capital cost for the GeneXpert unit (around 17,500 USD
per 4-module unit) is significantly higher than for microscopy
(around 1,500 USD per microscope) but much lower than for
conventional culture and DST (up to 1.4 million USD per new
laboratory or up to 300,000 USD per established laboratory,
given the need for extensive biosafety equipment and
infrastructure needed for conventional testing.
COST BENEFIT
Prof. Kwasi Addo, SON, UG Slide 69
MULTI AND EXTENSIVELYDRUG
RESISTANCE TB
Topic Five
Prof. Kwasi Addo, SON, UG Slide 72
73.
EXTENSIVELY DRUG RESISTANCETB
XDR-TB
Resistance to:
1. At least rifampicin and isoniazid (MDR-TB)
2. A fluoroquinolone
• Ciprofloxacin
• Ofloxacin
3. One or more of the following injectable drugs:
Aminoglycosides
• Kanamycin
• Amikacin
Polypeptide
• Capreomycin
Prof. Kwasi Addo, SON, UG Slide 73
74.
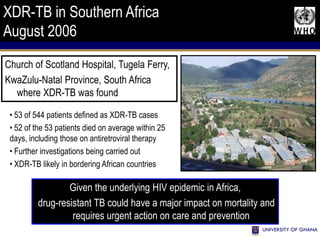
XDR-TB in SouthernAfrica
August 2006
• 53 of 544 patients defined as XDR-TB cases
• 52 of the 53 patients died on average within 25
days, including those on antiretroviral therapy
• Further investigations being carried out
• XDR-TB likely in bordering African countries
Church of Scotland Hospital, Tugela Ferry,
KwaZulu-Natal Province, South Africa
where XDR-TB was found
Given the underlying HIV epidemic in Africa,
drug-resistant TB could have a major impact on mortality and
requires urgent action on care and prevention
75.
CAUSES MDR TB
•Physician error
• Poor program performance
• Poor patient compliance
Ormerod LP. Br Med Bull 2005;73&74:17-24
Prof. Kwasi Addo, SON, UG Slide 75
NEW TREATMENT REGIMEN
FIXEDDOSE COMBINATIONS (FDCs)
Effective 1st June 2007
• DOTS Strategy: Directly Observed Treatment
Shortcourse
CATEGORY 1: For New smear positive, New smear negative
and Extra-pulmonary TB patients
2 months intensive phase: Ethambutol, Isoniazid,
Rifampicin and Pyrazinamide
4 months continuation phase: Isoniazid and
Rifampicin
2(HRZE) + 4(HR)
Prof. Kwasi Addo, SON, UG Slide 78
79.
TREATMENT 2
• CATEGORY2: For smear positive re-treatment cases
including:
- treatment failures
- treatment after default and
- relapses of smear positive cases
2(HRZE)S /1(HRZE) + 5HRE
Initial phase (3months) Continuation (5)
• CATEGORY 3: For uncomplicated cases of TB in children
2HR and Z +4HR
Prof. Kwasi Addo, SON, UG Slide 79
80.
TB PREVENTION &PROTECTION
TB
Prof. Kwasi Addo, SON, UG Slide 80
81.
PROPHYLAXIS
• BCG vaccination
•Pasteurization of milk
• Proper meat inspection
• Proper ventilation
• Avoiding MDR- XDR TB
Prof. Kwasi Addo, SON, UG Slide 81
82.
Keep windows open:
TBcannot
spread outside
or in fresh air
Prof. Kwasi Addo, SON, UG 82
83.
Live healthy:
• Eatright
• Get enough sleep
• Keep your
immune system
strong
Prof. Kwasi Addo, SON, UG 83
84.
ASSIGNMENT
• Discuss whycertain organisms are called acid-fast
organisms.
• Classify acid-fast bacteria and discuss their
pathogenicity.
Prof. Kwasi Addo, SON, UG 84
85.
References
• Cook G.C. and Zumla, A. (2005). Manson’s Tropical
Diseases, 21st Edn. China; W. B. Saunders.
Prof. Kwasi Addo, SON, UG Slide 85