1. The document describes skeletal muscle, including its classification, structure, properties, innervation and applied anatomy.
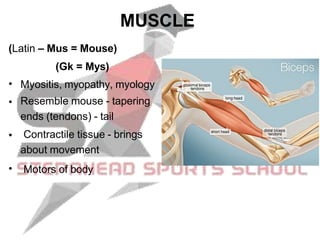
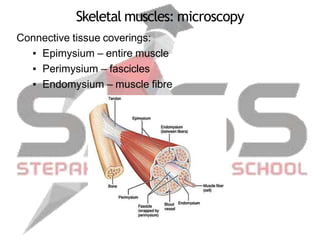
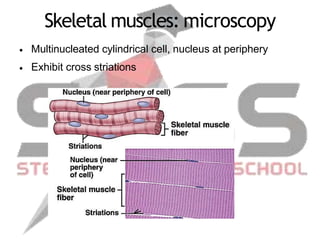
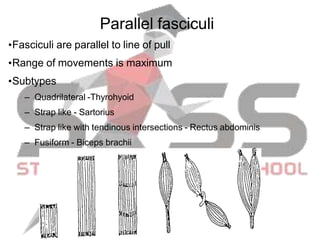
2. Key points include that skeletal muscle is striated, voluntary muscle attached to bones that acts as the motors of the body. It describes the fascicular architecture of muscles and how they are classified based on this.
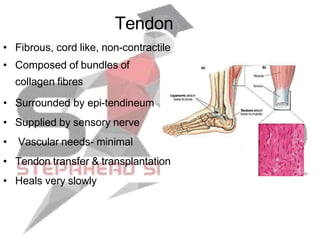
3. Laws of innervation and the concept of motor units are also explained. Applied anatomy discusses muscle paralysis, spasm, atrophy, hypertrophy and regeneration.