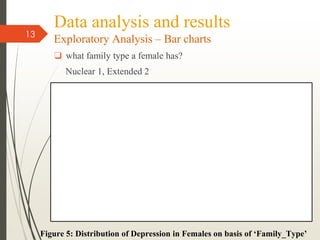
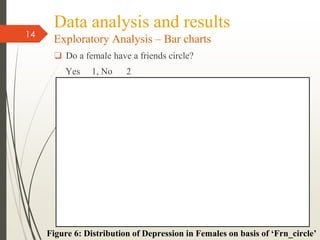
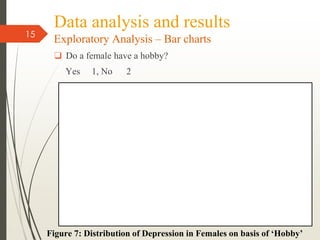
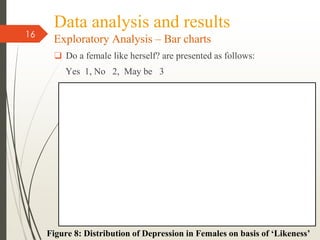
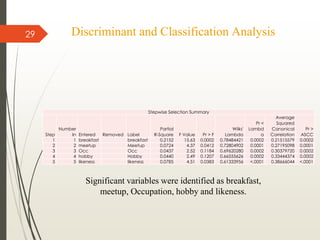
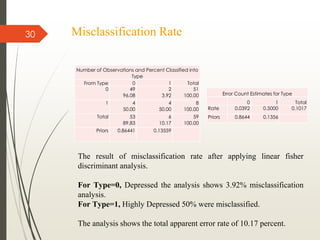
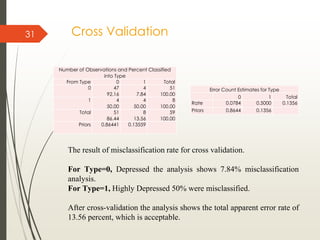
The document outlines a study analyzing factors that contribute to depression in females. It begins with an introduction on the rise of depression and aim of the study. A literature review covers previous research analyzing relationships between sleep, stressors, eating disorders, and depression. The data analysis section uses bar charts and factor analysis to explore relationships between depression and variables like breakfast intake, exercise, family type, and hobbies. Discriminant analysis identifies significant variables for classifying depression levels as breakfast habits, social activities, occupation, hobbies, and self-esteem. The study concludes that younger females and those with less social support are more susceptible to depression.