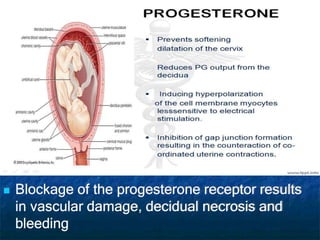
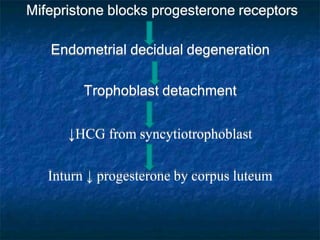
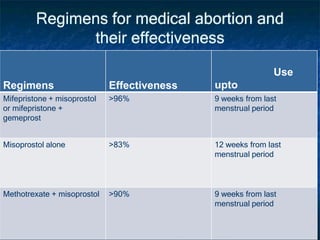
Medical termination of pregnancy can be performed using medication or surgically. Common medication methods include mifepristone with misoprostol or methotrexate with misoprostol. Surgical termination includes vacuum aspiration. The MTP Act of 1971 legalized abortion in India and established conditions for termination up to 20 weeks gestation. Termination requires consent and can be performed by qualified practitioners in approved facilities. The most effective and commonly used regimens include mifepristone followed by misoprostol 2-3 days later or methotrexate followed by misoprostol.