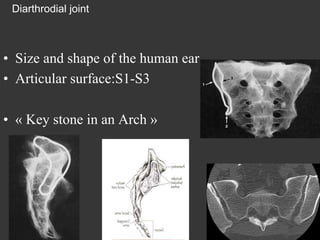
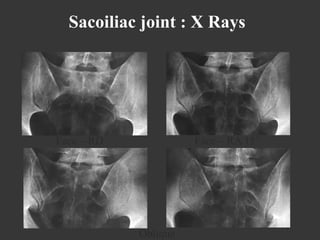
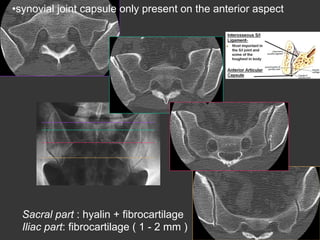
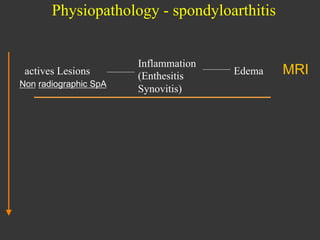
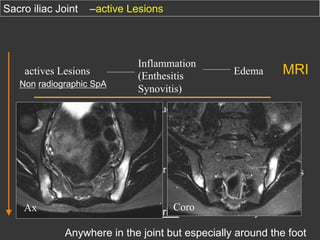
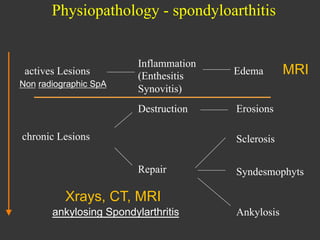
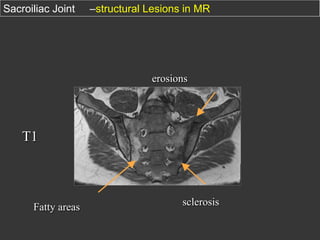
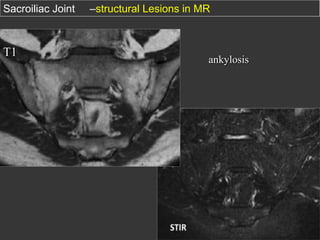
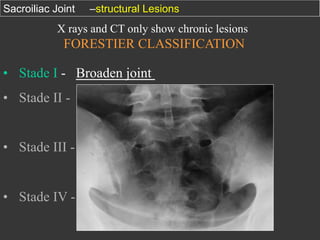
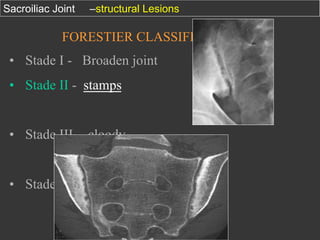
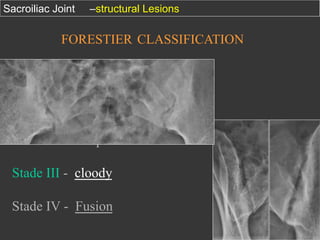
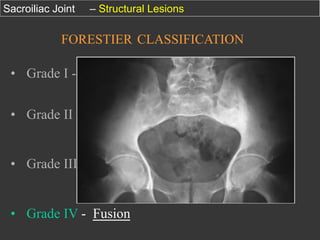
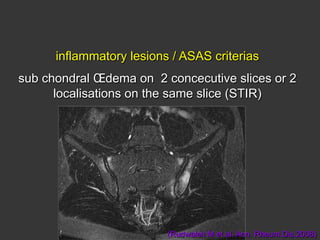
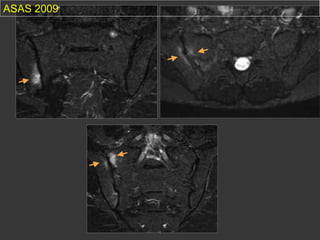
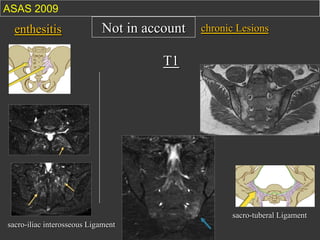
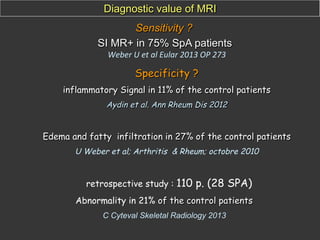
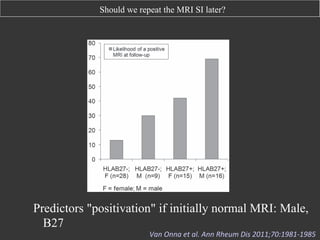
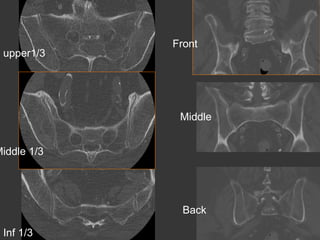
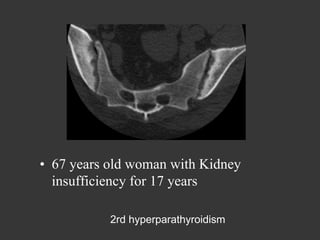
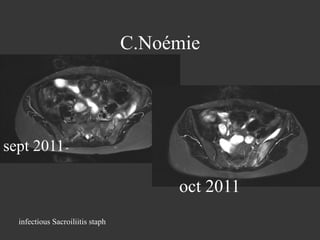
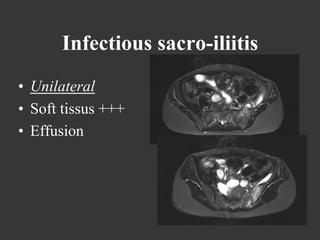
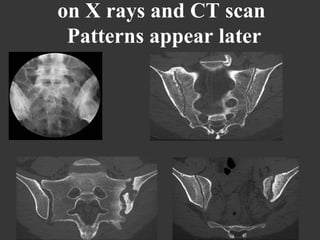
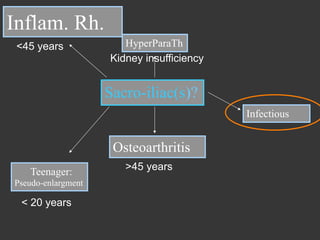
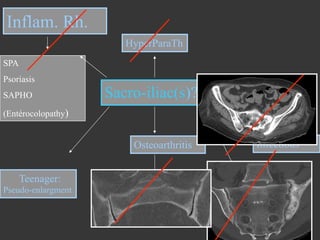
This document discusses imaging of the sacroiliac joint, including radiography and MRI findings. It begins with an overview of sacroiliac joint anatomy. It then describes common radiographic views and classifications of sacroiliac joint damage. The document focuses on using MRI to identify inflammatory lesions in the sacroiliac joints that can indicate early spondyloarthritis. It discusses how stopping NSAIDs before MRI may have little impact on findings. Repeating sacroiliac MRI months later generally does not reveal new cases, except possibly in HLA-B27 positive men. The document recommends sacroiliac MRI over spine MRI alone for axial spondyloarthritis workup given the low yield of isolated spinal findings without sac
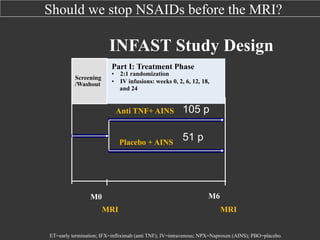
![Should make sacroiliac and / or spine MRI?
Patients avec atteinte axiale
symptomatique(n=362)
SA axiale nonradiologique (n = 160)
SA axiale radiologique =
SA (n = 202)
43,8 %
63,5 %
36,3 (10,3)
39,1 (11,3)
Duration of the ilness (ans) [DS]
5,7 (6,8)
11,2 (10,0)
BASDAI (0-10) [DS]
4,1 (2,0)
4,3 (2,0)
78,0 %
86,9 %
Males
Âge (ans) [DS]
HLA B27+
%
90
80
70
60
50
40
30
20
10
0
p
=
0,978
77,8
%
76,7
%
(112/144)
(132/172)
No
X
Rays
sign
of
sacroilii's
p
=
0,004
56,3
%
(54/96)
28,8
%
(17/59)
MRI
ac've
sacroilii's
Active MRI inflammatory
lesions spinal
Sacroilii's
seen
on
X
Rays
p
=
0,569
6,8
%
(3/44)
10,0
%
(6/60)
Active MRI inflammatory lesions
spinal (without sacroiliitis)
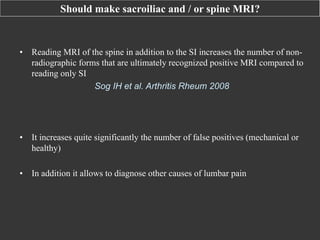
Whatever the clinical, sacroiliac MRI seems to be the most profitable review. Only
6.8% of non-radiological axial SA have isolated spinal inflammatory lesions
without sacroiliitis
Rudwaleit-‐
Song
-‐ACR
2010
-‐
(519)](https://image.slidesharecdn.com/msk-imaging-sacro-iliac-c-cyteval-min-131129100118-phpapp01/85/Msk-imaging-sacro-iliac-c-cyteval-35-320.jpg)



























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









