Here are the key steps I would take in managing this case:
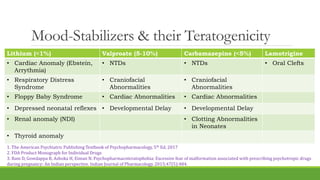
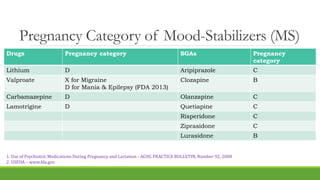
1. Discontinue valproate immediately given the high risk of teratogenicity.
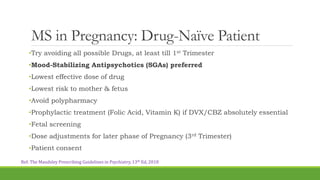
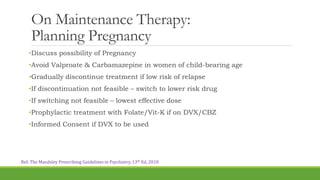
2. Discuss risks and benefits of continuing vs. discontinuing all medications with the patient and her family while also obtaining informed consent.
3. Given past unsatisfactory response to lithium and olanzapine, continuing treatment may be warranted despite risks to minimize risk of relapse.
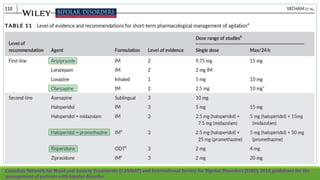
4. Switch to a safer alternative like lamotrigine or quetiapine, starting at a low dose and slowly titrating up under close monitoring.
5. Ensure folic acid supplementation, regular prenatal visits, and screening for fetal anomalies given past history