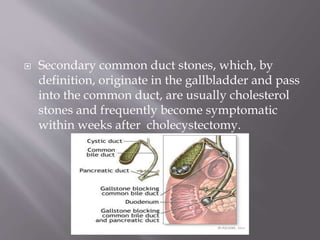
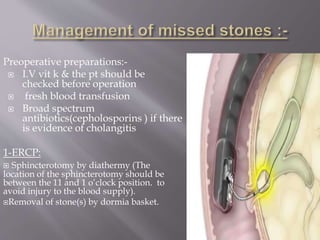
The document discusses residual common bile duct (CBD) stones following cholecystectomy. It notes that CBD stones occur in 5-10% of patients undergoing elective cholecystectomy and are usually seen within 6 weeks to 1 year later. ERCP is the definitive test for identifying CBD stones and options for removal include ERCP sphincterotomy, percutaneous lithotomy, extracorporeal lithotripsy, or surgical lithotomy if other options fail or are contraindicated. Surgical CBD exploration may involve opening the bile duct and milking out stones or flushing them out with saline via a catheter.