Download to read offline











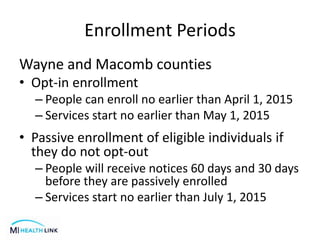
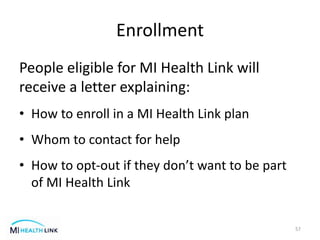
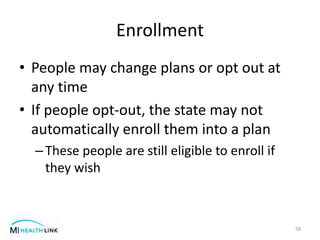


The MI Health Link program integrates Medicare and Medicaid benefits into a coordinated delivery system for eligible individuals in specific regions of Michigan. It offers various health services without co-payments or deductibles, emphasizing person-centered care and support. Enrollment begins in early 2015, with advisory committees and protections established for enrollees to ensure continuity of care and access to necessary services.



































































