2
Outline
• Primary Headachesoverview
• Pathophysiology of migraine
• Acute management
• Prophylactic management
• Case discussion
3.
3
What is aHeadache?
• Pain or discomfort affecting any part of the head arising from pain-
sensitive structures.
• Pain located in the head, above the orbitomeatal line and/or nuchal
ridge.
Headache
Facial Pain
4.
4
International Classification ofHeadache
Disorders (ICHD-3)
The ICHD-3 criteria defines three major categories of disorders:
• primary headaches
• secondary headaches
• cranial neuralgias and facial pain
5.
5
Primary Headaches
• Multipleentities causing episodic and chronic head pain/discomfort in
the absence of underlying medical conditions, medications or
traumatic injury.
• Primary headache disorders include:
• Migraine
• Tension-Type Headache(TTH)
• Trigeminal Autonomic Cephalalgias(TACS)
• Other primary headache disorders
7
Infrequent episodic TensionType Headache
(TTH)
Diagnostic criteria:
A. At least 10 episodes of headache occurring on <1 day/month on average (<12 days/year) and
fulfilling criteria B-D
B. Lasting from 30 minutes to 7 days
C. At least two of the following four characteristics:
A. bilateral location
B. pressing or tightening (non-pulsating) quality
C. mild or moderate intensity
D. not aggravated by routine physical activity such as walking or climbing stairs
D. Both of the following:
A. no nausea or vomiting
B. no more than one of photophobia or phonophobia
E. Not better accounted for by another ICHD-3 diagnosis
8.
8
Frequent episodic TTH
Diagnosticcriteria:
A. At least 10 episodes of headache occurring on 1-14 days/month on average for >3
months (≥12 and <180 days/year) and fulfilling criteria B-D
B. Lasting from 30 minutes to 7 days
C. At least two of the following four characteristics:
A. bilateral location
B. pressing or tightening (non-pulsating) quality
C. mild or moderate intensity
D. not aggravated by routine physical activity such as walking or climbing stairs
D. Both of the following:
A. no nausea or vomiting
B. no more than one of photophobia or phonophobia
E. Not better accounted for by another ICHD-3 diagnosis.
9.
9
Chronic TTH
Diagnostic criteria:
A.Headache occurring on ≥15 days/month on average for >3 months (≥180
days/year), fulfilling criteria B-D
B. Lasting hours to days, or unremitting
C. At least two of the following four characteristics:
A. bilateral location
B. pressing or tightening (non-pulsating) quality
C. mild or moderate intensity
D. not aggravated by routine physical activity such as walking or climbing stairs
D. Both of the following:
A. no more than one of photophobia, phonophobia or mild nausea
B. neither moderate or severe nausea nor vomiting
E. Not better accounted for by another ICHD-3 diagnosis.
10.
10
Trigeminal Autonomic Cephalalgias(TACs)
• A distinct set of headaches typified by shorter-lasting attacks of
unilateral intense pain in the trigeminal distribution with ipsilateral
cranial autonomic symptoms.
• Cluster headaches
• Paroxysmal hemicrania
• Short-lasting unilateral neuralgiform headache attack (SUNHA)
syndromes
• Hemicrania continua
11.
11
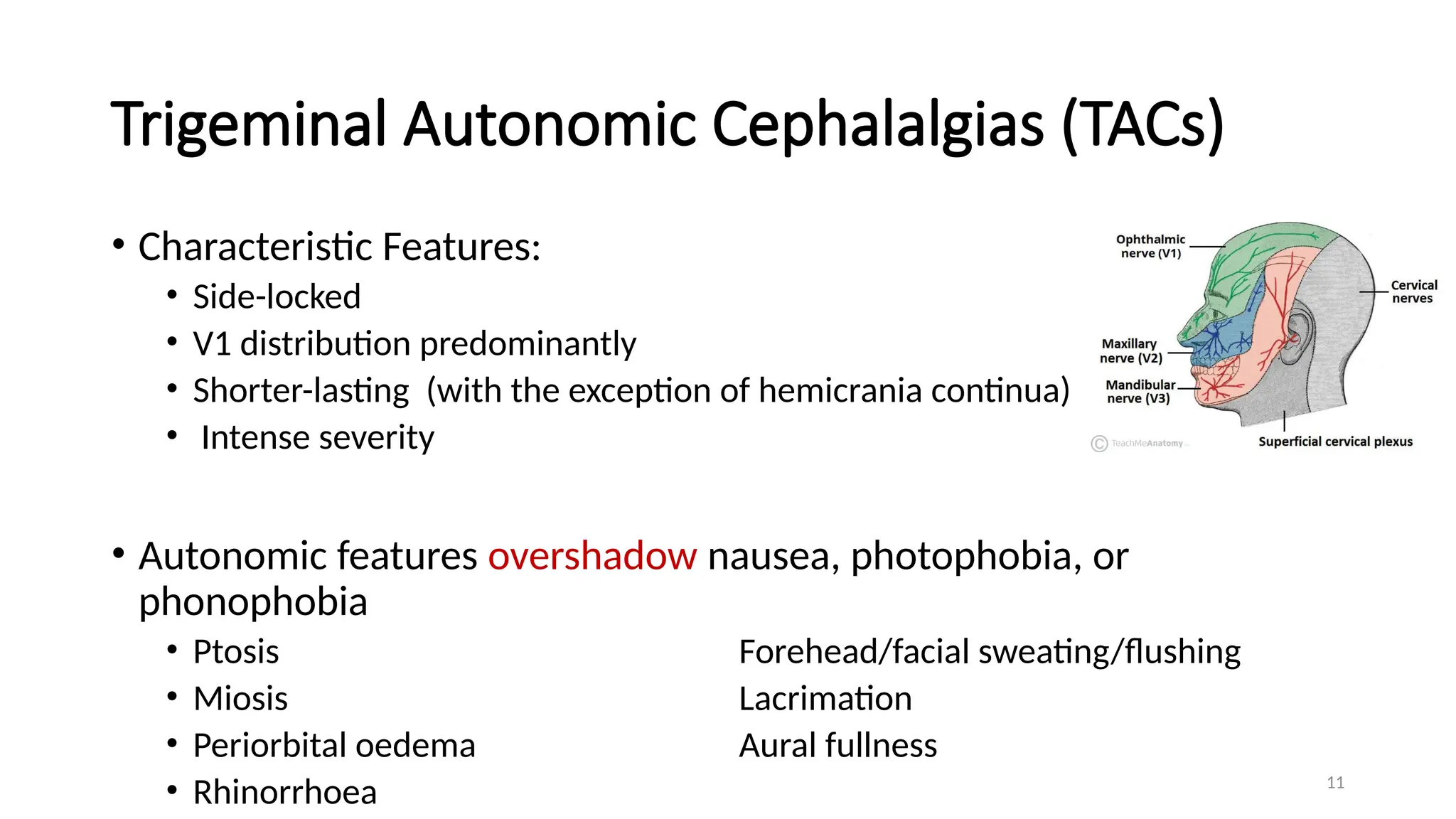
Trigeminal Autonomic Cephalalgias(TACs)
• Characteristic Features:
• Side-locked
• V1 distribution predominantly
• Shorter-lasting (with the exception of hemicrania continua)
• Intense severity
• Autonomic features overshadow nausea, photophobia, or
phonophobia
• Ptosis Forehead/facial sweating/flushing
• Miosis Lacrimation
• Periorbital oedema Aural fullness
• Rhinorrhoea
13
What are Migraines?
•A Migraine is a complex neurological
disorder characterized by recurrent
episodes of headaches mostly unilateral.
• It may be associated with visual, sensory,
motor, speech or brainstem symptoms—
collectively known as aura.
• Aura may arise most often before the head
pain but that may occur during or afterward
the headache.
15
What are Migraines?
•Africa has an estimated fifty-six million people living with migraine.
• World-wide prevalence is approximately 14-15 %
• African studies report 5-10%
• Male to female ratio of approximately 1:3
16.
16
Classification of Migraine
•Migraine without aura (formerly, common migraine)
• Probable migraine without aura
• Migraine with aura (formerly, classic migraine)
• Probable migraine with aura
• Episodic migraine
• Chronic migraine
• Chronic migraine associated with analgesic overuse
• Childhood periodic syndromes that may not be precursors to or
associated with migraine - these syndromes include cyclic vomiting,
abdominal migraine, and benign paroxysmal vertigo of childhood.
17.
17
IHS Classification –ICHD 3:Migraine with aura
The following criteria must be met:
One or more visual, sensory, speech, motor, brainstem, or retinal symptoms, as
well as at least 2 of the following 4 criteria:
(1) at least 1 aura symptom spreading gradually over 5 or more minutes and/or 2
or more symptoms occurring in succession
(2) each aura symptom lasting 5–60 minutes
(3) at least 1 aura symptom being unilateral
(4) the aura being accompanied by or followed shortly by headache
(5) Not better accounted for by another ICHD-3 diagnosis.
18.
18
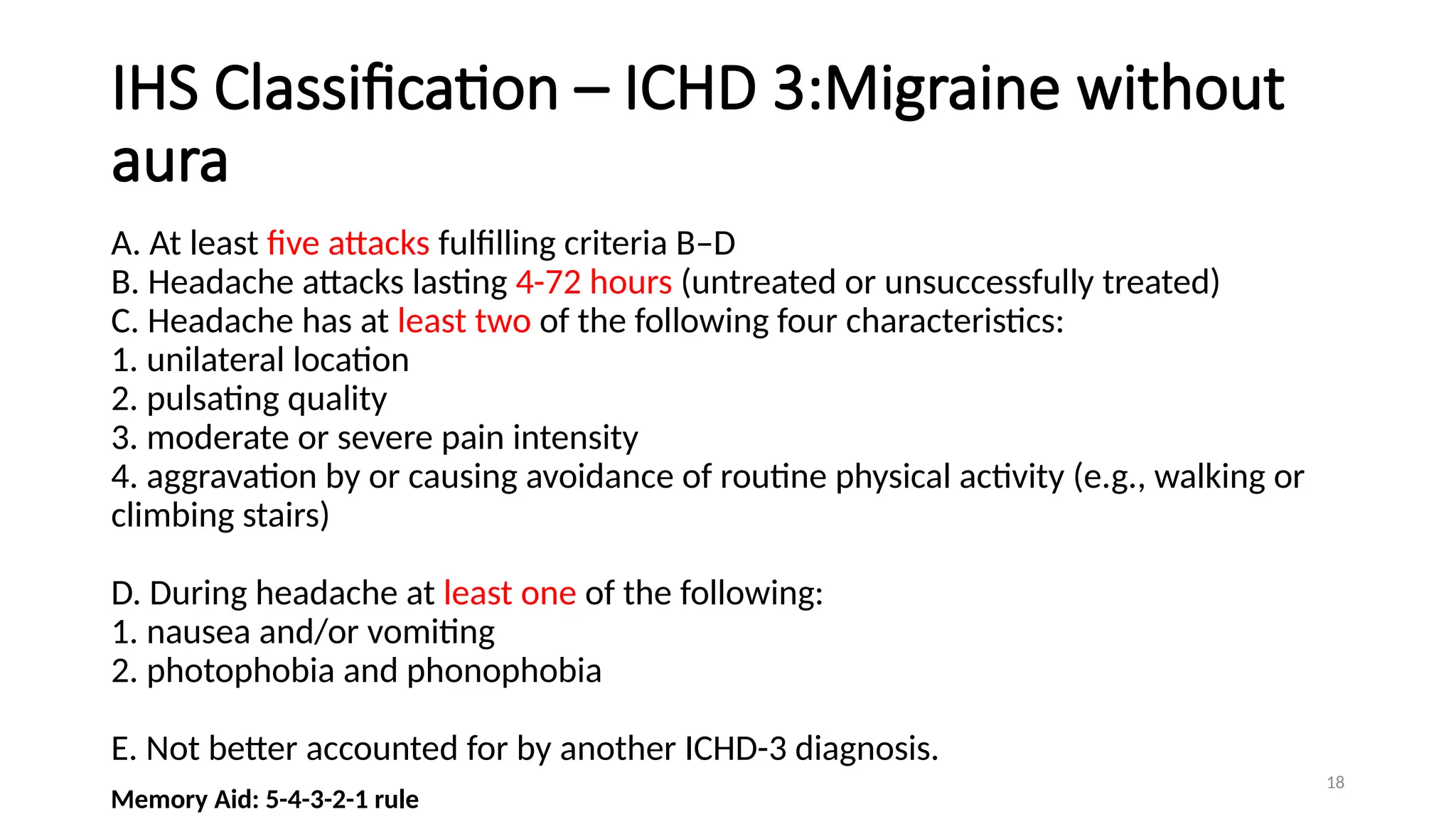
IHS Classification –ICHD 3:Migraine without
aura
A. At least five attacks fulfilling criteria B–D
B. Headache attacks lasting 4-72 hours (untreated or unsuccessfully treated)
C. Headache has at least two of the following four characteristics:
1. unilateral location
2. pulsating quality
3. moderate or severe pain intensity
4. aggravation by or causing avoidance of routine physical activity (e.g., walking or
climbing stairs)
D. During headache at least one of the following:
1. nausea and/or vomiting
2. photophobia and phonophobia
E. Not better accounted for by another ICHD-3 diagnosis.
Memory Aid: 5-4-3-2-1 rule
19.
19
Migraine classification andvariants
• Chronic migraine : > 15 days a month for 3 consecutive months with 8 of
days fulfilling migraine criteria.
• Episodic migraine: < 15 days a month
• Status migrainosus: migraine lasting more than 72hours
• Ophthalmoplegic migraine: 3rd
nerve palsy, ptosis, ocular muscle paralysis .
• Hemiplegic migraine.
• Migraine equivalent (acephalgic): aura without migraine. Seen in persons
with recurrent headaches, mostly older than 40.
20.
20
Pathophysiology
The key structuresinvolved in migraine include:
• the large intracranial vessels, dura mater and
peripheral terminals of the trigeminal nerve that
innervate these structures (the trigeminovascular
complex)
• the caudal portion of the trigeminal nucleus, which
extends into the dorsal horns of the upper cervical
spinal cord and receives input from the first and
second cervical nerve roots (the trigeminocervical
complex)
• rostral pain-processing regions, such as the
ventroposteromedial thalamus and the cortex .
• the pain-modulatory systems in the brain that
modulate input from trigeminal nociceptors at all levels
of the pain-processing pathways.
22
Pathophysiology
• Genetically susceptible/
hyperexcitable brain
• ?Cortical spreading depression
• Calcitonin Gene-Related Peptide
• Substance P
• Neurokinin A
• Nitric Oxide
• Serotonin
• Cyclic adenosine
monophosphate
Oguzhan et al, Migraine and neuroinflammation, the inflammasome perspective, J. Headache Pain,22:55(2021)
23.
23
Acute Management
• Oncea diagnosis of migraine has been established, it is important to
assess the extent of a patient’s disease and disability.
• The Migraine Disability Assessment Score (MIDAS) is a well-validated,
easy-to-use tool.
• Assessment and management of associated comorbidities is key.
PHQ2, PHQ9, MSQ, SF-36
25
Acute Management –Patient education
Patient education is an important aspect of migraine management.
• It is helpful for patients to understand that migraine is an inherited tendency to
headache
• that migraine can be modified and controlled by lifestyle adjustments and medications
• it cannot be eradicated;
• except in women with migraine with aura on oral estrogens or combined oral
contraceptives, migraine is not associated with serious or life-threatening illnesses.
(migraine with aura : 2-3-fold increase in strokes)
Curtis KM et al. Use of combined oral contraceptives among women with migraine and non-migrainous headaches. 2006;73:189-194. doi 10.1016/ j.contraception. 2005.08.009
26.
26
Acute Management –Non-pharmacologic
HEADACHE DIARY AVOID TRIGGERS HEALTHY DIET REGULAR EXERCISE REGULAR SLEEP
PATTERNS
AVOIDANCE OF
EXCESS CAFFEINE
AND ALCOHOL
AVOIDANCE OF
ACUTE CHANGES IN
STRESS LEVELS
27.
27
Acute Management- Pharmacologic
•Judicious use of appropriate medications
• The optimal regimen is individualized and depends on a number of
factors: severity of the attack being key.
• Mild migraine attacks can usually be managed by oral agents
( the average efficacy rate is 50–70%).
• Severe migraine attacks may require parenteral therapy.
28.
28
Acute Management- Pharmacologic
Theideal acute/abortive medication should have/provide:
• minimal / no adverse effects
• Little requirement for repeat dosing
• complete/ near-complete relief from pain
• freedom from disruptions to daily routine
31
Level A (establishedefficacy) if two high-quality studies support efficacy.
Level B (probably effective) if one good-quality or two lower-quality studies support efficacy.
Level C (possibly effective) if one lower-quality or two lowest-quality studies support efficacy.
Level U (data inadequate or conflicting) if studies are conflicting or available studies are insufficient quality to contribute to knowledge.
33
Acute Management- Emergency
•Parenteral administration of drugs such as dihydroergotamine and sumatriptan is
approved by the FDA for the rapid relief of a migraine attack.
• Peak plasma levels of dihydroergotamine are achieved
• 3 min after IV dosing,
• 30 min after IM dosing,
• 45 min after SC dosing.
• If an attack has not already peaked, SC or IM administration of 1 mg dihydroergotamine
suffices for about 80–90% of patients.
• Sumatriptan, 6 mg SC, is effective in 70–80% of patients.
∼
34.
34
Acute management- Emergency
•Drug absorption is impaired during migraine because of reduced gastrointestinal
motility.
• Delayed absorption occurs even in the absence of nausea and is related to the
severity of the attack and not its duration.
• When oral NSAIDs and/or triptan agents fail, the addition of a dopamine
antagonist such as metoclopramide 10 mg should be considered to enhance
gastric absorption.
• Parenteral dopamine antagonists (e.g: chlorpromazine, prochlorperazine,
metoclopramide) can also provide significant acute relief of migraine in
combination with parenteral 5-HT1B/1D agonists.
• A common IV protocol used for the treatment of severe migraine is the
administration over 2 min of a mixture of 5 mg of prochlorperazine and 0.5 mg of
dihydroergotamine.
35.
35
Acute Management –Narcotic use
• Narcotics are effective in the acute treatment of migraine eg : IV pethidine (50–100mg) in
the emergency room.
• This regimen is clearly suboptimal for patients with recurrent headache.
• Narcotics do not treat the underlying headache mechanism; rather, they act to alter the
pain sensation.
• Narcotic addiction can greatly confuse the treatment of migraine. Narcotic craving and/or
withdrawal can aggravate and accentuate migraine.
• It is recommended that narcotic use in migraine be limited to patients with severe, but
infrequent, headaches unresponsive to other pharmacologic approaches.
36.
36
Acute Management: Triptanuse
Contraindications:
• Uncontrolled hypertension
• Ischaemic heart disease
• Peripheral Artery Disease
• History of stroke
• Hemiplegic migraine
• **Allow at least a 24-hour interval after Dihydroergotamine(DHE) use to use a
triptan.
37.
37
Acute Management: Triptanuse
• 7 oral triptans currently available
• Varying onset of action and duration
Memory Aid: R-E-S-Z-A-N-F Onset of Action Duration of Effect
• Rizatriptan fastest shortest
• Eletriptan
• Sumatriptan
• Zolmitriptan
• Almotriptan
• Naratriptan
• Frovatriptan slowest longest
38.
38
Acute Management: Triptanuse
• One dose for early/mild headache.
• Dose may be repeated after 2 hours if headache recurs. (Max oral dose in 24
hours: 200mg)
• Limit use to no more than 2-3 days / week to prevent medication overuse
headaches.
• May be used concurrently with NSAIDS/opioids and anti-emetics (dopamine
antagonists)
• If response less than desired for one triptan, a different triptan may be tried.
39.
39
Medication overuse headache
•Not a separate headache entity
• Associated with Acute medications overuse (> 15 days/month for simple
analgesics/NSAIDS, >10 days/month for triptans and opioids)
• Propensity to aggravate headache frequency and induce a state of refractory
daily or near-daily headache called medication- overuse headache.
40.
40
Medication overuse headache
Treatment:Breaking The Cycle
• Stopping culprit medications versus gradual taper
• Symptoms will worsen before they get better
• Withdrawal symptoms: nervousness, restlessness, nausea, vomiting, insomnia,
constipation (may last 2 to 10 days or several weeks)
• May require admission
• Bridging therapy / emergency parenteral treatment
• Initiating prophylactic therapy
Prevention
• Use of non-pharmacological therapies for acute attacks
• Limiting use of acute therapies to no more than 2-3 days per week.
41.
41
Prophylactic Management
Preventive therapiesare among the most powerful tools available to improve the
well-being of people with migraine.
• reduction in attack frequency
• reduce the severity or duration of headache attacks
• reduce the need for acute treatment
• improve efficacy of acute treatments
• reduced disability
• improved quality of life
• A reduction in headache frequency of 50% or more is considered a good
response to treatment.
42.
42
Prophylactic management
• Priorto development of Calcitonin Gene-Related Peptide (CGRP) monoclonal
antibodies, only one medication (methysergide: semi-synthetic ergot alkaloid,
5HT2 antagonist, 5HT1 agonist) had been developed specifically for migraine
prevention.
• Methysergide withdrawn o/a fibrosis(retroperitoneal, pleural, subendocardial)
and cardiac valve dysfunction.
• Migraine prevention is therefore a secondary/off-label indication for most drugs
currently in use as oral preventive agents.
• Many such medications are efficacious as migraine preventives.
43.
43
Prophylactic management- indications
Twosevere or disabling or four less disabling migraine attacks per
month
Acute migraine treatment ineffective or contraindicated
Medication-overuse headache present
Highly disabling migraine attacks (e.g., hemiplegic migraine or migraine
with brainstem aura)
Patient preference
44.
44
Prophylactic Management –AHS/AAN 2021
• Level A (established as effective) if two high-quality studies support efficacy.
• Level B (probably effective) if one good-quality or two lower-quality studies.
• support efficacy, Level C (possibly effective) if one lower-quality or two
lowest-quality studies support efficacy.
• Level U (data inadequate or conflicting) if studies are conflicting or available
studies are insufficient quality to contribute to knowledge.
51
Prophylactic management
• Theprobability of success with any one of the antimigraine drugs is 50–75%.
• Many patients are managed adequately with low-dose amitriptyline,
propranolol, topiramate, gabapentin, or valproate.
• Once effective stabilization is achieved, the drug is continued for 6 months and
∼
then slowly tapered to assess the continued need.
• Many patients can discontinue medication and experience fewer and milder
attacks with long periods of pain freedom.
55
Migraine in Children:Modified ICHD-3 criteria
Migraine without Aura
• Headache duration: headache attacks lasting 2 to 72 hours
(when untreated or unsuccessfully treated)
• Headache location: can be unilateral or bilateral
• Associated features: photophobia and phonophobia can be
inferred from behavior
56.
56
Migraine in Children
Maypresent as:
• colic in infants:
• Recurrent episodes of irritability, fussing, or crying from birth to 4 months of
age
• No concern for failure to thrive
• Crying episodes
• More than 3 times a week
• For 3 or more hours per day
• For at least 3 weeks
• Cyclical vomiting
• Abdominal migraine
57.
57
Migraine in Children
PracticeGuidelines for preventive and acute treatment of migraine in children. American Academy of Neurology in Practical Neurology: Migraine in Children. May 2019
58.
58
Migraine in children
HotopA, Ferguson M, Ask the PharmD: What are the recommendations for preventing and treating pediatric migraine? Pract Pain Manag. 2020;20(2)
59.
59
Migraine in Pregnancy
•Approximately one half to three-fourths of female migraineurs experience
improvement in migraine with a significant reduction in the frequency and
intensity of their attacks during the second and third trimester of pregnancy.
• Women who have migraines with aura are at greater risk for having more
frequent migraines during pregnancy.
• Most of the recommended drugs for migraine prophylaxis are FDA pregnancy
category C, D or even X as there are no specific clinical trials evaluating drug
treatment of migraine during pregnancy and breastfeeding.
• Nonpharmacologic options must be first line before drug therapy.
60.
60
• Category A
Adequateand well-controlled studies have failed to demonstrate a risk to the fetus in the first trimester of
pregnancy (and there is no evidence of risk in later trimesters).
• Category B
Animal reproduction studies have failed to demonstrate a risk to the fetus and there are no adequate and
well-controlled studies in pregnant women.
• Category C
Animal reproduction studies have shown an adverse effect on the fetus and there are no adequate and
well-controlled studies in humans, but potential benefits may warrant use of the drug in pregnant women
despite potential risks.
• Category D
There is positive evidence of human fetal risk based on adverse reaction data from investigational or
marketing experience or studies in humans, but potential benefits may warrant use of the drug in pregnant
women despite potential risks.
• Category X
Studies in animals or humans have demonstrated fetal abnormalities and/or there is positive evidence of
human fetal risk based on adverse reaction data from investigational or marketing experience, and the risks
61.
61
Migraine in Pregnancy
Acute/AbortiveTherapy:
• Acetaminophen safe in all trimesters
• NSAIDs may be used ONLY in the second trimester
• Triptans are category C
Preventive Therapy:
• Consider prophylactic medication when the benefit of migraine prophylaxis for
the mother and fetus is determined to be significantly higher than the risk
associated with using prophylactic medications.
62.
62
Contraindicated medications inPregnancy
• Calcitonin Gene Related Peptide(CGRP) monoclonal antibodies
• Flunarizine
• Topiramate
• sodium valproate
• zonisamide
• MIG-99(extract of the herb feverfew).
63.
63
Summary
• Migraine canbe modified and controlled by lifestyle adjustments and
medications. it cannot be eradicated.
• Pharmacologic treatment is individualized! One size does NOT fit all.
• It is recommended that narcotic use in migraine be limited to patients with
severe, but infrequent, headaches unresponsive to other pharmacologic
approaches.
• Except in women with migraine with aura on oral estrogens or combined oral
contraceptives, migraine is not associated with serious or life-threatening
illnesses. (migraine with aura : 2-3-fold increase in strokes).
• Women of child-bearing age should be counselled about medications with
teratogenic side effects and appropriate contraceptives.
• Prophylactic medications reduce frequency and severity of migraine
• Assessing comorbidities and migraine disability objectively helps improve quality
of life of migraineurs.
66
Q 1.
1.Which ofthe following symptoms suggests a primary cause
of headaches?
a.Occurring regularly with menstrual cycle
b.Photophobia
c. Diplopia
d.Worse on laying supine
67.
67
Q 2.
1.The followingsubstances are involved in migraine
pathophysiology except:
a.Acetylcholine
b.Serotonin
c. Estrogen
d.Calcitonin Gene Related Peptide
68.
68
Q 3.
1.Management ofMigraine encompasses all the following
but:
a.Headache diary
b.Regular exercise
c. Trigger management
d.Alcohol use
69.
69
Q 4.
1.Which ofthe following is a migraine-specific abortive
treatment?
a.Paracetamol
b.Sumatriptan
c. Amitriptyline
d.Caffeine
70.
70
Q 5.
1.Which ofthe following describes preventive/prophylactic
treatment for migraine?
a.Should be taken at onset of migraine attack
b.Should be taken daily for a specified period of time
c. Should be taken as and when the headache gets worse
d.Should be prescribed without considering comorbidities.
72
Case 1
• 40-year-oldfemale, A.B
• Banker, married with 2 children
• Asthmatic, BMI of 32
• Starting experiencing migraine as a teenager, worsened over past few years
• Has headaches 4 days per week in the past 6 months
• Takes a combination of acetaminophen/aspirin/caffeine for headaches
• She has developed abdominal pains from regular use of the medication.
73.
73
Case 1
• Left– sided headaches over the past 48hrs of 6/10 severity with nausea,
photophobia and phonophobia.
• She has been prescribed sumatriptan in the past by her primary care doctor.
• Currently has to take maximum daily doses sumatriptan with little response.
• She is still having headaches 4 days a week despite taking sumatriptan
• She wants to be pain-free .
• She feels guilty about “ignoring her children” as she stays away from them when her
headaches are bad.
74.
74
Case 1- Questions
1.How will you classify A.B’s migraines?
2. What are her comorbidities
3. What medications MUST you avoid?
4. Which medications will you consider for acute/abortive treatment?
5. Which medications will you consider for prophylactic/preventive treatment?
75.
75
Case 1- Answers
1.Chronic migraine without aura
2. Asthma, obesity, NSAID-induced gastritis
3. Avoid beta blockers, NSAIDs , medications associated with weight gain.
4. Sumatriptan + dopamine antagonist; alternative triptan; alternative route of
administration- sc /nasal; ergot derivatives.
5. Topiramate**; amitriptyline; valproic acid**; botulinum toxin
Keep a headache diary, Look for triggers: avoid/modify, at onset of headaches
DO NOT COMBINE TRIPTANS AND ERGOTS
**Medications with teratogenic effects. Caution on effective contraception
76.
76
Case 2
• 28-year-oldfemale, EM, online marketer, works on her own schedule.
• Single
• BMI – 26
• On combined oral contraceptive pills.
• Headache last night of 8/10 severity, right sided, associated with nausea and a
tingling sensation running down her right arm in the first hour of the headache.
• Had to turn off the television and room lights to enable her sleep.
77.
77
Case 2
• Misseda planned evening out with her friends to celebrate a graduation.
• Headache persists this morning at 6/10 severity.
• Has had 3 similar episodes over the past 2 years relieved by ibuprofen.
• Current episode is not responding to ibuprofen.
• She denies any stressors but has been having poor sleep because of her neighbor’s
dogs barking throughout the night the past week.
78.
78
Case 2
1. Howwill you classify E.M’s migraines?
2. What are her comorbidities
3. What medications MUST you avoid?
4. Which medications will you consider for acute/abortive treatment?
5. Which medications will you consider for prophylactic/preventive treatment?
79.
79
Case 2- Answers
1.Episodic migraine with aura (sensory)
2. Use of combined oral contraceptive pills (COCPs) in migraine with aura is
associated with increased risk of stroke.
3. Switch COCPs to progestin-only or alternatives contraception e.g. IUD.
4. Her headaches are moderate to severe in intensity and infrequent. Find out when
during the headache she takes ibuprofen. Should be taken at onset of pain.
Alternatives: acetaminophen/aspirin/caffeine; opioids+ dopamine antagonist;
triptans +/-NSAIDs +/-dopamine antagonists, ergots, gepants, ditans.
5. Not a candidate for Prophylaxis
#3 It’s a common and often cardinal manifestation of a myriad of diseases, and may be a disease unto itself,
Pain referred to the forehead, orbits, temples or scalp. Does not usually cover pain isolated to the face or neck.
#22 CGRP (Intrinsically involved in migraine pathogenesis, Belongs to calcitonin family, Expressed in subset of small neurons in vagus, trigeminal and dorsal root ganglion)
#58 CHAMP study – amitriptyline, topiramate and placebo. Terminated early for futility o/a similar outcomes at 6 months