


































![“ I conclude that though the individual physician is not perfectible, the system of care is, and that the computer will play a major part in the perfection of future care systems.” Clem McDonald, MD NEJM 295:1355, 1976 Thank you! Blackford Middleton, MD [email_address]](https://image.slidesharecdn.com/middletoncgu2005v6-1221618587084240-8/75/Middleton-Cgu2005v6-61-2048.jpg)

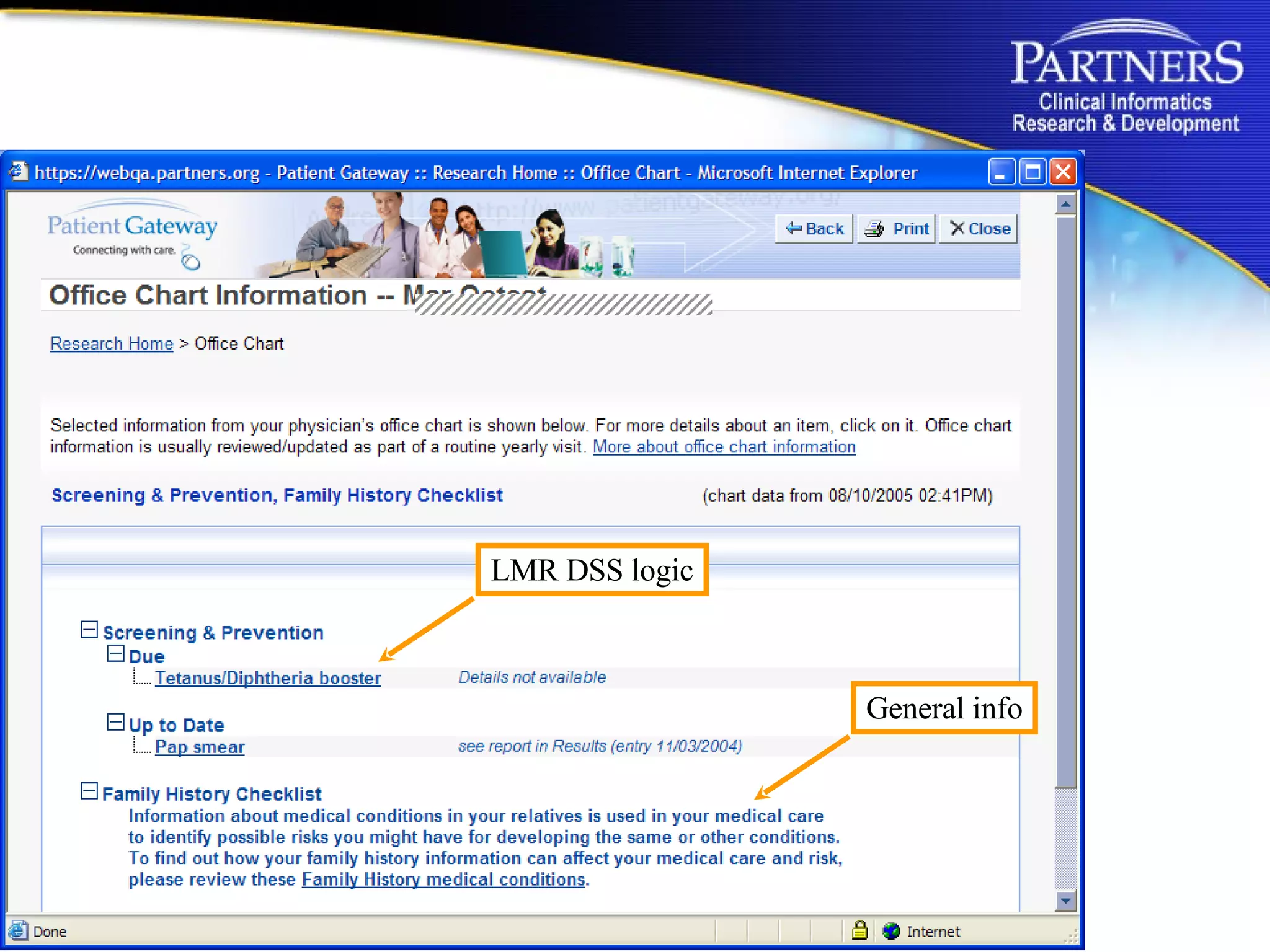
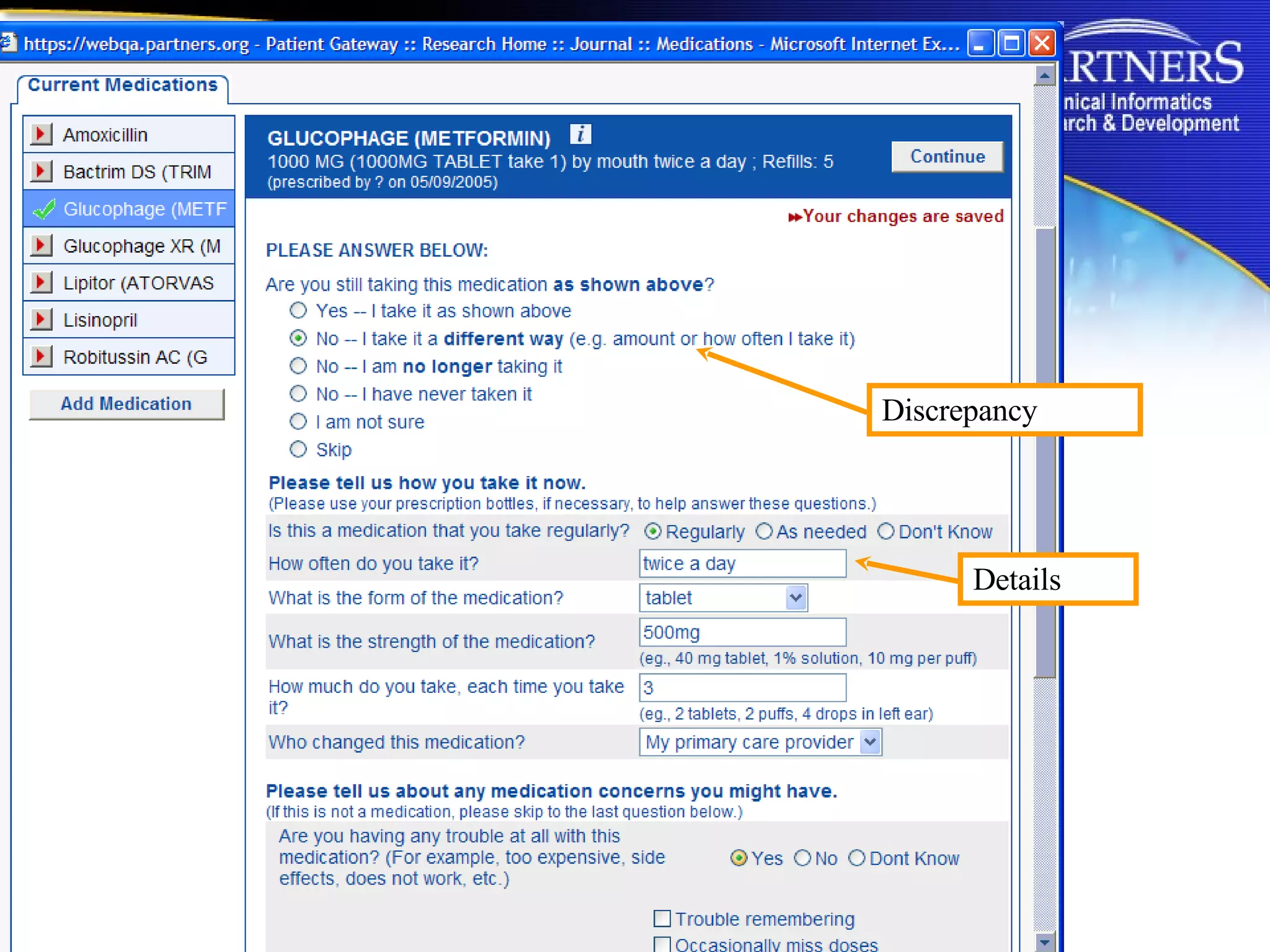
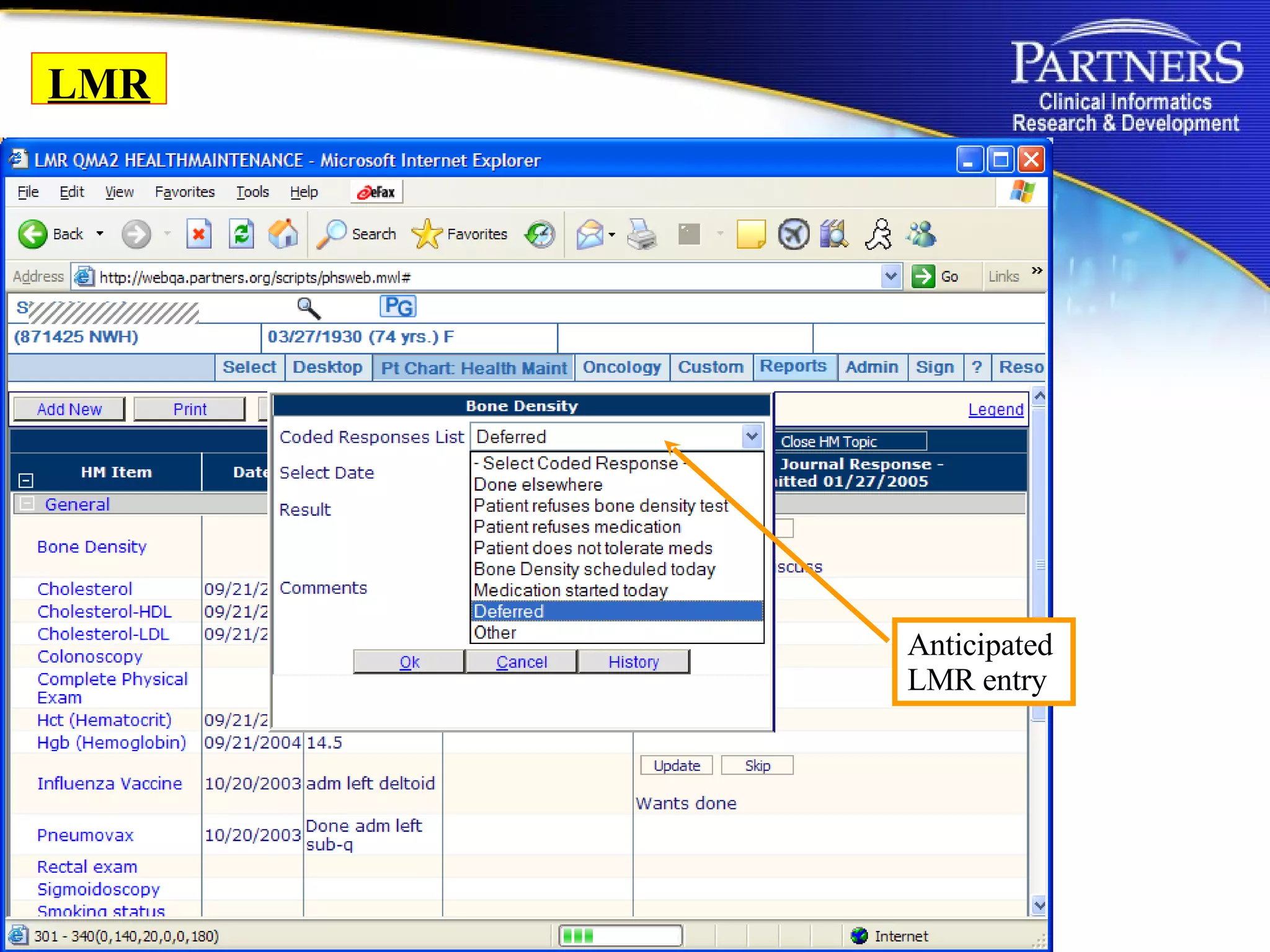
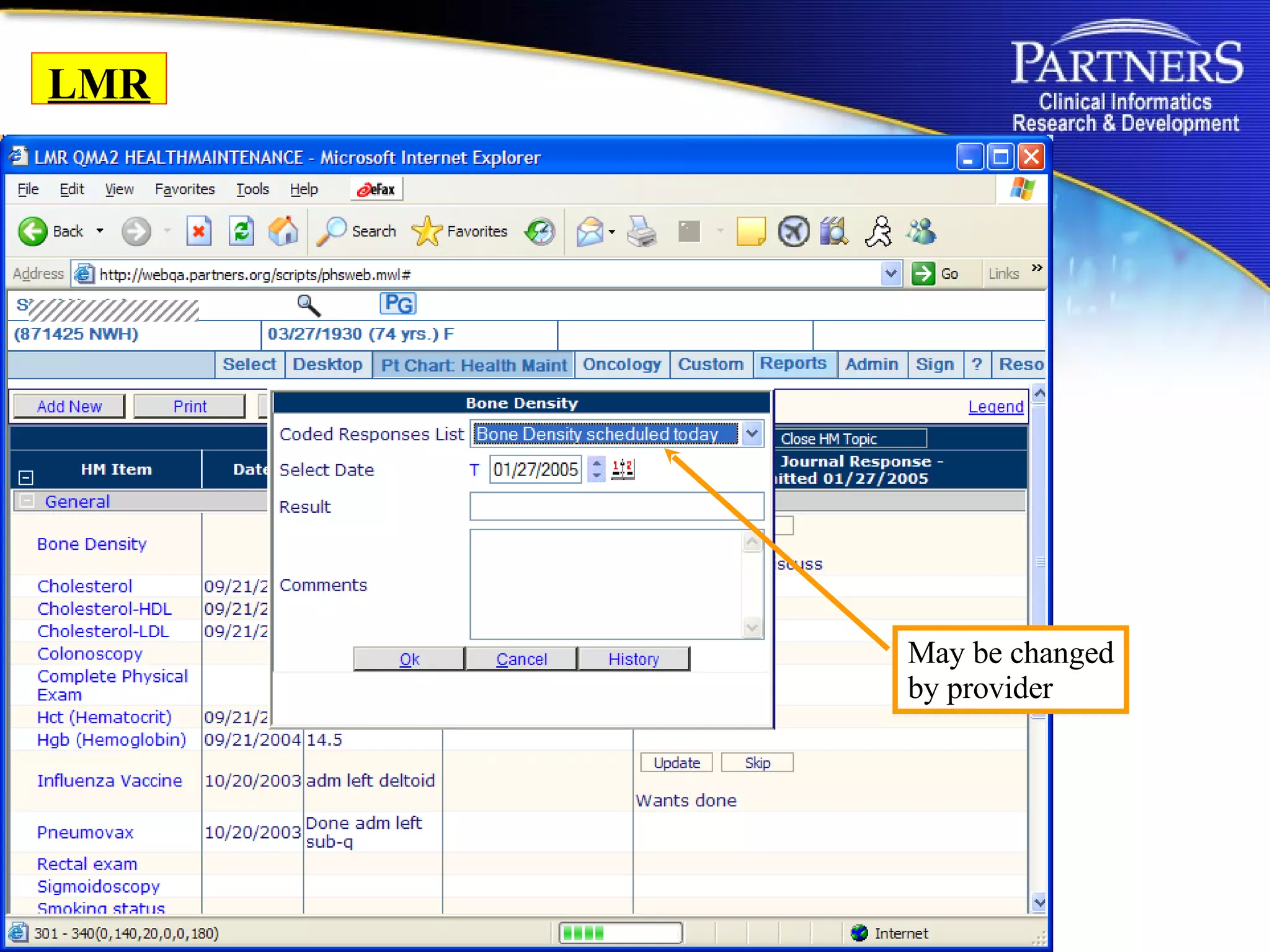
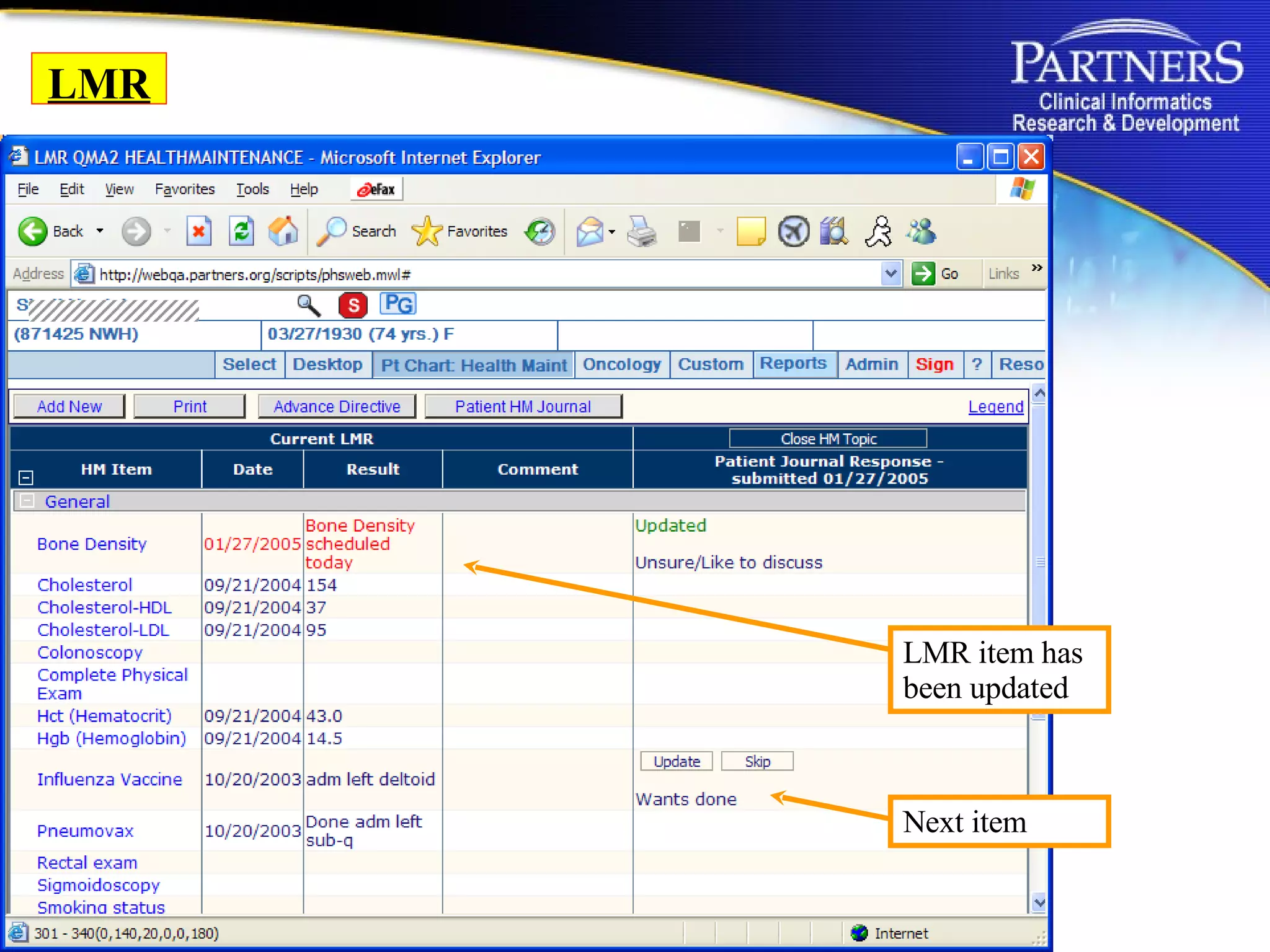
The document summarizes the Partners HealthCare Patient Gateway, which allows patients to access their medical information online. It discusses how the gateway aims to address issues like medical errors due to a lack of access to patient information. It also notes that the gateway is part of Partners HealthCare's efforts to improve patient-centered care by better engaging and informing patients.










































































