INTRODUCTION
Occupational therapy canbe described as
the art and the science of channeling an
individual's effort in specially selected activities
that have been designed to restore and
enhance his performance. Occupational
therapy facilitates the learning of a wide
variety of skills and functions that are essential
to well developed human adaptation.
3.
• Occupation isan activity or set of activities that is
performed with some consistency and regularity,
that brings structure, and is given value and
meaning by individuals and a culture.
• Activity is a set of tasks with a specific end point
or outcome that is greater that of any constituent
task. Task is a set of actions having an end point
or a specific outcome.
• Action is a set of voluntary movements or mental
processes that form a recognizable and purposeful
pattern (grasping, holding, pulling, pushing,
turning, kneeling, standing, walking, thinking,
remembering, smiling, chewing, winking, etc)
4.
DEFINITION
Occupational therapy isthe application
of goal-oriented, purposeful activity in the
assessment and treatment of individuals
with psychological, physical or
developmental disabilities.
5.
GOAL
The main goalis to enable the patient to
achieve a healthy balance of occupations through the
development of skills that will allow him to function at
a level satisfactory to himself and others.
6.
PRINCIPLES
• Select theactivities based on interest IQ levels
strengths and abilities of the client.
• Utilizes the client’s available resources.
• Select short duration activities to foster a sense
of accomplishment and enhance self-
confidence.
• Provide good reinforcement for even small
achievements.
• Plan and selected activities that gives new
experience for the client to meet the day to day
activities.
7.
POINTS TO BEKEPT IN MIND
1.The patient should be involved as much as possible
in selecting the activity
2.Select an activity that interests or has the potential to
interest him
3.The activity should utilize the patient's strengths and
abilities
4.The activity should be of short duration to foster a
feeling of accomplishment.
5.If possible, the selected activity should provide some
new experiences for the patient.
8.
6.Occupational therapy mustarouse and sustain the
patient's interest.
7.In initial act the goal must not be too far from each
other.
8.Individuals should be given activities according to
age and capabilities.
9.The work should be progressive in skill, difficulty
and complexity.
10.The standard of the expected work performance
must be based on the capacity of patient and not on
other people's standard.
11.Encouragement (not criticism) should be used.
10.
SETTINGS
Occupational therapy isprovided to children,
adolescents, adults and elderly patients. These
programs are offered in
Psychiatric hospitals
Nursing homes
Rehabilitation centers
Special schools
Community group homes
Community mental health centers
Day care centers
Halfway homes
De-addiction centers
11.
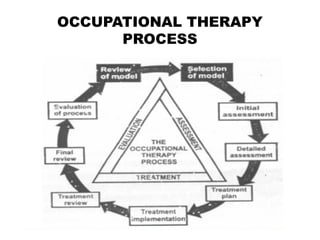
OCCUPATIONAL THERAPY PROCESS
Theoccupational therapy process fall into
three main stages:
1. Assessment
2. Treatment and intervention
3. Evaluation
Selecting a model is also an integral step that must
occur at the beginning of the process. Illustrates this
relationship, highlighting the three main stages in a
triangle but also giving prominence to the essential
first stage of selecting a model.
12.
Thus occupational therapyis related to these four
main stages:
1. Selecting a model
2. Assessment
3. Treatment/Intervention
4. Evaluation
1. Selecting aModel
The occupational therapy process is a circular one.
A model is selected to translate the occupational
therapy paradigm into practice in a particular work
setting or with an individual client.
For example an acute psychiatric setting might
normally use model of human occupation, but it may
be more appropriate to use a psychodynamic model
with certain clients.
Each stage of assessment and treatment is related
to the chosen model, but it’s appropriate scan only
be judged by evaluating the outcome of the process.
15.
Selection of anappropriate model is the first stage of
occupational therapy process. Many influence the
choice of model used in a particular area of practice.
More than one model be used in a particular setting
or it may be possible to use only one. Some of these
models have been extensively used.
The four models within each frame of reference are
briefly mentioned here:
(i) Activity therapy: It is from the adaptive
performance frame of reference. This model, first
presented by Mosey in the early 1970s, was one of
the first attempts to bring together theories, goals of
intervention and methods in a unifying framework.
16.
(ii)Occupational therapy asa communication
Process: It is from the psychodynamic frame of
reference, this model was developed by Fiddler and
Fiddler in the 1960s.
When individual and group psychotherapy were being
widely used for the treatment of all type of psycho
logical dysfunction, and it is still the most
comprehensive model of occupational therapy for use
in this field.
17.
(iii) Facilitating growthand development from the
development frame of reference: This model is
based on the theories of human development aspect
of development theory which are drawn on for most
occupational therapy models. But Loren's model of
facilitating growth and development is most explicit
about the developmental nature of occupational
therapy.
(iv)A Model of Human Occupation: It is from the
occupational behaviour frame of reference. This
model, first presented by Kielhofner, Burke and Igi in
1980, is based on general system theory, theories of
motivation and role theory.
18.
2. Assessment
Assessment isthe basis for all intervention
and must be both thorough and valid in order to
ensure that treatment is appropriate. Assessment
in two stages:
(i). Initial assessment
(ii). Detailed assessment
19.
Assessment begins fromthe moment a referral is
received or, if specific referrals are not made in a
particular setting from the moment the therapist starts
to identify those clients who could benefit from
occupational therapy.
Initial assessment is a screening process to
determine the main problem area of the client and
whether or not occupational therapy can be of any
value in this case. Once the client is accepted for
treatment a detailed assessment is carried out to
determine his needs, assets, interests and goals.
20.
3. Treatment
There maybe no clear division between
assessment and treatment in occupational therapy
where clients are often assessed by being observed in
activities. Treatment in three stages, which may be
repeated as necessary, depending on the client's
progress:
1. Formulation of treatment plan
2. Treatment implementation
3. Treatment review
21.
The therapist andclient formulate the preliminary
treatment plan together. The plan includes goals of
treatment, methods to be used, an individual
programme and a list of the people who need to be
informed about the programme.
The treatment plan is put into practice and the
client's progress is continuously monitored. Regular
reviews are held to evaluate the need for major
programme changes. After the review the treatment
plan is updated, including the programme of activities.
22.
4. Evaluation
The circularprocess of occupational therapy is
completed by the three stages of evaluation:
(i). Final treatment review
(ii). Evaluation of process
(iii). Review of model
The final review of the client's progress is used to
reach decisions about discharge or referral, to other
agencies. Evaluation of the process should go on
throughout the occupational therapy programme.
Evaluation may lead to change in any part of the
occupational therapy process.
23.
Paradigm changes areunlikely to occur at
this level. Evaluation and quality assurance
methods are similar as to evaluate effectiveness of
any interventions. decisions about discharge or
referral, to other agencies. Evaluation of the
process should go on throughout the occupational
therapy programme.
Evaluation may lead to change in any part of
the occupational therapy process. Paradigm
changes are unlikely to occur at this level.
Evaluation and quality assurance methods are
similar as to evaluate effectiveness of any
interventions.
24.
Process of Intervention
Itconsists of six stages:
1. Initial evaluation of what patient can do and
cannot do in a variety of situations over a period
of time.
2. Development of immediate and long-term goals by
the patient and therapist together. Goals should be
concrete and measurable so that it is easy to see
when they have been attained.
3. Development of therapy plan with planned
intervention.
25.
4. Implementation ofthe plan and monitoring the
progress. The plan is followed until the first evaluation.
If found satisfactory it is continued and altered, if not.
5. Review meetings with patient and all the staff
involved in treatment.
6. Setting further goals when immediate goals have
been achieved; modifying the treatment program as
relevant.
26.
TYPES OF ACTIVITIES
(i)Diversionalactivities: These activities are
used to divert one's thoughts from life stresses or
to fill time. For example, organized games.
(ii)Therapeutic activities: These activities are
used to attain a specific care plan or goal. For
example, basket making, carpentry, etc.
27.
Suggested Occupational Activitiesfor
Psychiatric Disorders
(i)Anxiety disorder: Simple concrete tasks with no
more than 3 or 4 steps that can be learnt quickly. For
example, kitchen tasks, washing sweeping, mopping,
mowing lawn and weeding gardens.
(ii)Depressive disorder: Simple concrete tasks which
are achievable; it is important for the patient to
experience success. Provide positive reinforcement
after each achievement. For example, crafts, mowing
lawn, weeding gardens.
28.
(iii) Manic disorder:Non-competitive activities that
allow the use of energy and expression of feelings.
Activities should be limited and changed frequently.
Patient needs to work in an area away from
distractions. Example, raking grass, sweeping, etc.
(iv) Schizophrenia (paranoid): Non-competitive,
solitary meaningful tasks that require come degree
of concentration so that less me is available to focus
on delusions. For example, puzzles, scrabble, etc.
29.
(v)Schizophrenia (catatonic): Simpleconcrete tasks
in which patient is actively involved. Patient needs
continuous supervision, and at first works best on a
one-to-one basis. For example, metal work, molding
clay, etc.
(vi)Antisocial personality: Activities that enhance
self-esteem and are expressive and creative, but not
too complicated. Patient needs supervision to make
sure each task is completed. For example, leather
work, painting, etc.
30.
(vii)Dementia: Group activitiesto increase feeling
of belonging and self-worth. Provide those
activities which promote familiar individual
hobbies. Activities need to be structured, requiring
little time for completion and not much
concentration. Explain and demonstrate each task,
then have patient repeat the demonstration. For
example, cover making, packing goods, etc.
31.
Childhood and AdolescentDisorders
•Children: Playing, storytelling, painting, poetry,
music, etc.
•Adolescents: Creative activities such as leather
work, drawing, painting.
•Mental retardation: Repetitive work assignments
are ideal provide positive reinforcement after each
achievement. For example, cover making, candle
making, packaging goods, etc.
•Substance abuse: Group activities in which
patient uses his talents. For example, involving
patient in planning social activities, encouraging
interaction with others, etc.
32.
Occupational Therapy ServiceCenter
The services are provided to children, adolescent,
adults and the elderly of all functional groups and
diagnostic categories, in institutional, community
based, partial hospitalization, residential treatment
and Forensic Programs.
These Programs are offered in:
(i) Psychiatric hospitals
(ii) Nursing homes
(iii) Psychosocial and rehabilitation centers
33.
(iv) Sheltered workshopsor clinics
(v) Public and private schools
(vi) Group homes or correctional institutions
(vii) Home health agencies
(viii)Community mental health centres
(ix) Day care centres
(x) Private practice or physician's office
(xi) Industry and business establishment etc.
34.
Occupational therapy toenhance sensory
integration
Sensory-integrative therapy provides systematic
and controlled therapy to remediate the underlying
neural dysfunction. Enhancement of sensory-
integrative function should promote more effective and
adaptive occupational performance.
Aims:
To normalize sensory integration and therefore
normalize motor and perceptual responses.
35.
Technique:
Non-competitive pleasurable activitiesare used
to reduce anxiety, which interferes with sensory
integration in the reticular and limbic systems by
producing over-arousal.
Treatment :
1. Activities Kicking and throwing balls
2. Rolling Crawling
3. Scooter board
4. Hopping
5. Skipping
6. Jumping
36.
Occupational Therapy forDeveloping
Cognitive Skills
It is given to increase the capacity of the patient
to perform tasks competently and to fulfill his normal
life roles.
Aims:
1. To restore the lost skills; for example,
practicing cookery after a head injury
2. To use remaining skills to compensate for the
loss; for example, learning to make lists to
compensate for loss of memory
37.
3. To makeadjustments in life-style so that the lost
skills are not needed; for example, moving into a
hostel where meals will be provided.
Cognitive skills are taught as an integral part of
achieving competence in occupational performance.
Treatment Activities:
1. Crafts, which are useful for developing
concentration, creative thinking and planning.
2. Quizzes and table games, for developing
concentration, memory, and problem-solving skills.
3. Art and poetry, for developing creative
thinking and imagination.
38.
4. Play-reading ordiscussion, to develop
language skills, concentration and memory
5. Creative writing, to develop creative thinking,
language skills and concept formation
6. Reality orientation, to develop memory,
attention, concentration and orientation
39.
ADVANTAGES
• Helps todevelop social skills and provide an
outlet for self-expression.
• Strengthens ego defenses.
• Develops a more realistic view of the self in
relation to others.
40.
ROLE OF NURSE
•Coordinates with other therapeutic team
members in diagnosing the abilities, strengths,
and talents, interests IQ levels of the client and
in selecting the activity for a specific client
• Provides a series of graded experiences to the
client, e.g. observing the demonstration of any
activity to more direct and active experiences
• Educates the client to develop specific new skills
• Encourages socialization and exhibits positive
interest to the client
• Guides the client in formulation of new hobbies
by strengthening the abilities of the client
41.
• Appreciates ifthe client performs any approved
behavior.
• Offers tokens for each accomplishment of the
work, based on the principle of positive
reinforcement.
• Helps the client to develop independent living
skills.
• Approaches community agencies for job
placement of the clients in approved social
activities.
• Assists in developing good social interaction and
relationship.
• Never criticizes the client, when he is performing
any activity.















![MHN [OT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mhnot-221104092133-da8d1872-thumbnail.jpg?width=640&height=640&fit=bounds)










































