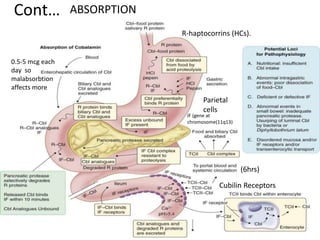
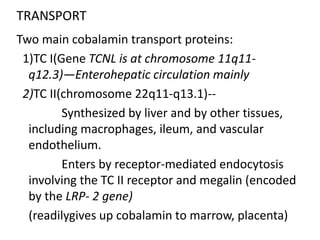
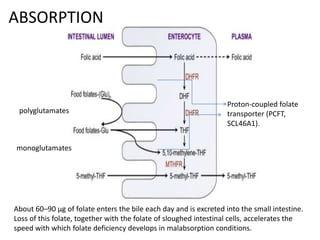
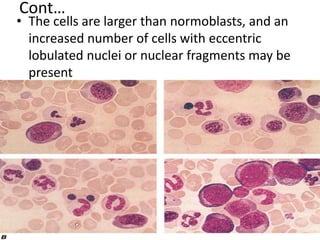
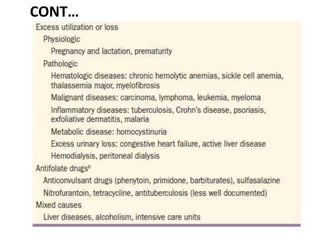
This document discusses megaloblastic anemias caused by cobalamin and folate deficiencies. It covers the absorption, transport, biochemical functions and deficiencies of cobalamin and folate. The key clinical features of megaloblastic anemia are described, including neurological manifestations. Causes, hematological and bone marrow findings, ineffective hematopoiesis, and treatment approaches are summarized. Lifelong cobalamin injections are usually needed to treat deficiency, while folate deficiency responds to oral supplementation.