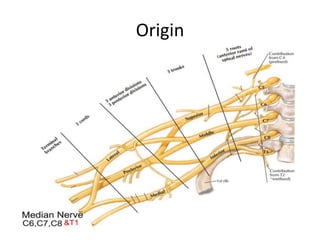
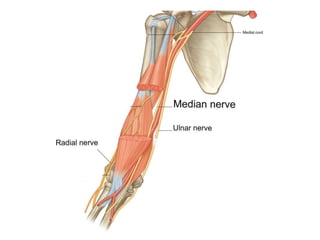
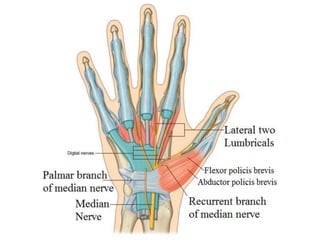
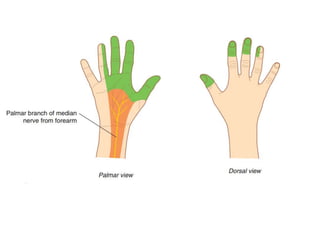
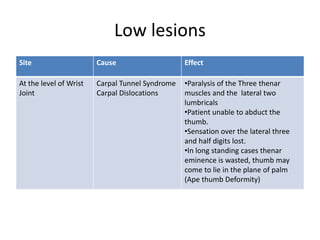
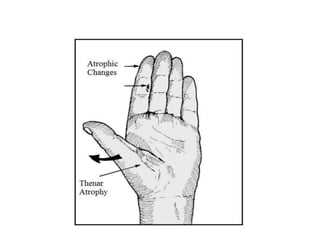
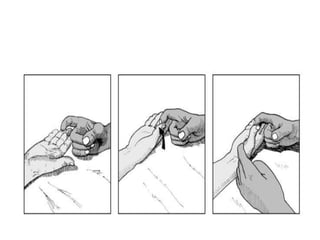
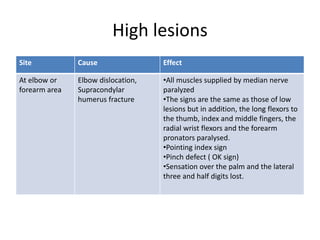
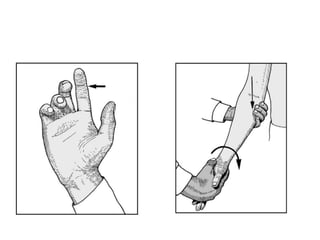
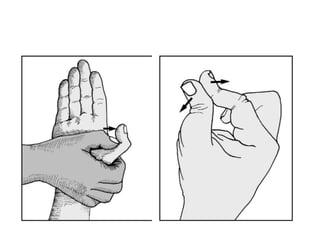
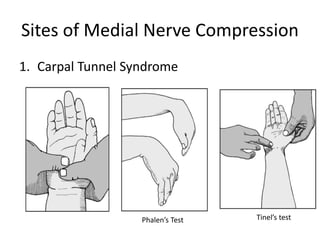
The median nerve originates in the arm, enters the forearm between the two heads of the pronator teres muscle, and passes through the carpal tunnel into the hand. In the forearm, it gives off branches including the anterior interosseous nerve and palmar cutaneous branch. In the hand, it divides into a recurrent branch and palmar digital branches. Injuries can occur at the wrist (carpal tunnel syndrome), elbow, or forearm, causing paralysis of muscles in the hand and loss of sensation in the palm and fingers. The median nerve is susceptible to compression in the carpal tunnel, at the pronator teres, and from anterior interosseous nerve syndrome.