Download to read offline

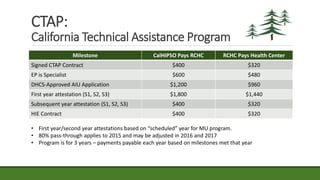
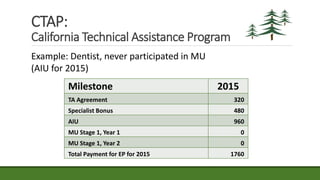
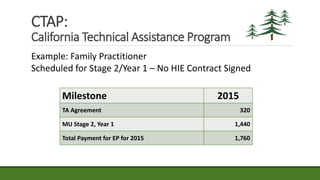
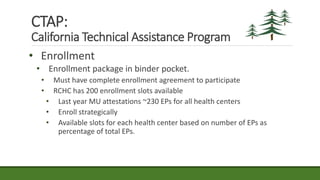
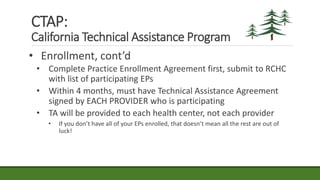
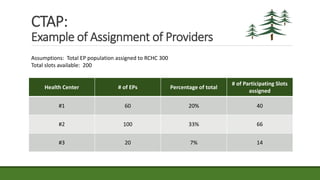













The document provides an agenda and information about an upcoming Meaningful Use Mini-Camp on October 21, 2015. The agenda includes introductions, an overview of the California Technical Assistance Program (CTAP), a review of the 2015-2017 Modification Final Rule, a discussion of challenging measures, and strategic planning for Meaningful Use. Additional details are then provided about CTAP funding, milestones, and payments. The document concludes with sections on enrollment in CTAP and an overview of some of the most challenging Meaningful Use measures.









![New clinical quality measure reporting in Practice Fusion [slides]](https://cdn.slidesharecdn.com/ss_thumbnails/junecqmwebinarslideshare-140611132004-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)











































![Cms+ehr incentive program_hospital_training_final[1]](https://cdn.slidesharecdn.com/ss_thumbnails/cmsehrincentiveprogramhospitaltrainingfinal1-101130114653-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)





