Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Mastoiditis imaging poster (1)
Similar to Mastoiditis imaging poster (1) (20)
Mastoiditis imaging poster (1)
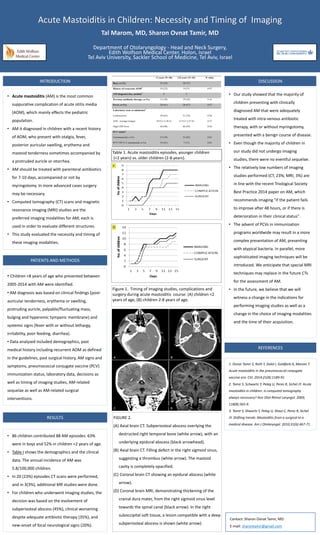
- 1. <2 years (N=46) 2-8 years (N=42) P-value Boys, n (%) 25 (54) 30 (71) History of recurrent AOM1 10 (22) 9 (21) 0.97 AM diagnosis day, median2 4 5 Previous antibiotic therapy, n (%) 13 (28) 19 (45) 0.16 Fever, n (%) 28 (61) 28 (67) 0.57 Laboratory tests at admission3 Leukocytosis ANC, average (range) High CRP level 29 (63) 10.9 (1.5-26.5) 44 (98) 31 (74) 11.9 (1.2-27.8) 40 (95) 0.28 0.37 0.92 PCV status4 Unimmunized, n (%) PCV7/PCV13 immunized, n (%) 27 (59) 19 (41) 35 (83) 7 (17) 0.01 0.01 INTRODUCTION • Acute mastoiditis (AM) is the most common suppurative complication of acute otitis media (AOM), which mainly effects the pediatric population. • AM it diagnosed in children with a recent history of AOM, who present with otalgia, fever, posterior auricular swelling, erythema and mastoid tenderness sometimes accompanied by a protruded auricle or otorrhea. • AM should be treated with parenteral antibiotics for 7-10 days, accompanied or not by myringotomy. In more advanced cases surgery may be necessary. • Computed tomography (CT) scans and magnetic resonance imaging (MRI) studies are the preferred imaging modalities for AM; each is used in order to evaluate different structures. • This study evaluated the necessity and timing of these imaging modalities. PATIENTS AND METHODS • Children <8 years of age who presented between 2005-2014 with AM were identified. • AM diagnosis was based on clinical findings (post- auricular tenderness, erythema or swelling, protruding auricle, palpable/fluctuating mass, bulging and hyperemic tympanic membrane) and systemic signs (fever with or without lethargy, irritability, poor feeding, diarrhea). • Data analyzed included demographics, past medical history including recurrent AOM as defined in the guidelines, past surgical history, AM signs and symptoms, pneumococcal conjugate vaccine (PCV) immunization status, laboratory data, decisions as well as timing of imaging studies, AM-related sequelae as well as AM-related surgical interventions. DISCUSSION • Our study showed that the majority of children presenting with clinically diagnosed AM that were adequately treated with intra-venous antibiotic therapy, with or without myringotomy, presented with a benign course of disease. • Even though the majority of children in our study did not undergo imaging studies, there were no eventful sequelae. • The relatively low numbers of imaging studies performed (CT, 23%; MRI, 3%) are in line with the recent Triological Society Best Practice 2014 paper on AM, which recommends imaging "if the patient fails to improve after 48 hours, or if there is deterioration in their clinical status" . • The advent of PCVs in immunization programs worldwide may result in a more complex presentation of AM, presenting with atypical bacteria. In parallel, more sophisticated imaging techniques will be introduced. We anticipate that special MRI techniques may replace in the future CTs for the assessment of AM. • In the future, we believe that we will witness a change in the indications for performing imaging studies as well as a change in the choice of imaging modalities and the time of their acquisition. Contact: Sharon Ovnat Tamir, MD E-mail: sharontamir@gmail.com REFERENCES 1. Ovnat Tamir S, Roth Y, Dalal I, Goldfarb A, Marom T. Acute mastoiditis in the pneumococcal conjugate vaccine era. CVI. 2014;21(8):1189-91. 2. Tamir S, Schwartz Y, Peleg U, Perez R, Sichel JY. Acute mastoiditis in children: is computed tomography always necessary? Ann Otol Rhinol Laryngol. 2009; 118(8):565-9. 3. Tamir S, Shwartz Y, Peleg U, Shaul C, Perez R, Sichel JY. Shifting trends: Mastoiditis from a surgical to a medical disease. Am J Otolaryngol. 2010;31(6):467-71. Acute Mastoiditis in Children: Necessity and Timing of Imaging Tal Marom, MD, Sharon Ovnat Tamir, MD Department of Otolaryngology - Head and Neck Surgery, Edith Wolfson Medical Center, Holon, Israel Tel Aviv University, Sackler School of Medicine, Tel Aviv, Israel Table 1. Acute mastoiditis episodes, younger children (<2 years) vs. older children (2-8 years). Figure 1. Timing of imaging studies, complications and surgery during acute mastoiditis course: (A) children <2 years of age, (B) children 2-8 years of age. RESULTS • 86 children contributed 88 AM episodes. 63% were in boys and 52% in children <2 years of age. • Table I shows the demographics and the clinical data. The annual incidence of AM was 5.8/100,000 children. • In 20 (23%) episodes CT scans were performed, and in 3(3%), additional MR studies were done. • For children who underwent imaging studies, the decision was based on the evolvement of subperiosteal abscess (45%), clinical worsening despite adequate antibiotic therapy (35%), and new-onset of focal neurological signs (20%). FIGURE 2. (A) Axial brain CT. Subperiosteal abscess overlying the destructed right temporal bone (white arrow), with an underlying epidural abscess (black arrowhead). (B) Axial brain CT. Filling defect in the right sigmoid sinus, suggesting a thrombus (white arrow). The mastoid cavity is completely opacified. (C) Coronal brain CT showing an epidural abscess (white arrow). (D) Coronal brain MRI, demonstrating thickening of the cranial dura mater, from the right sigmoid sinus level towards the spinal canal (black arrow). In the right suboccipital soft tissue, a lesion compatible with a deep subperiosteal abscess is shown (white arrow). A