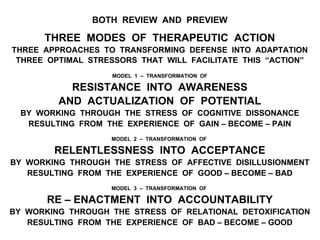
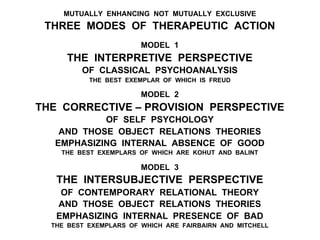
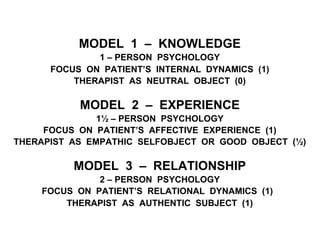
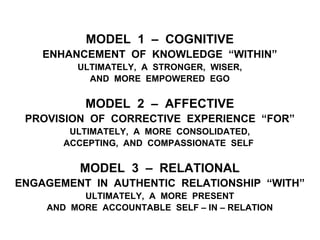
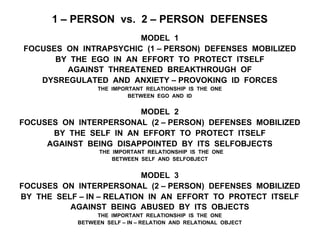
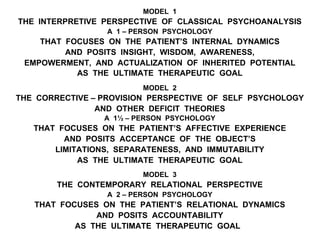
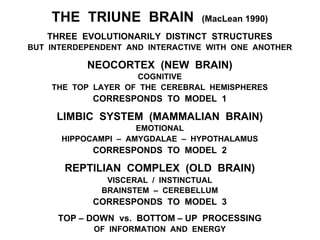
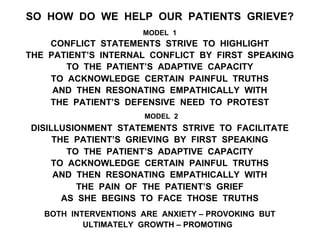
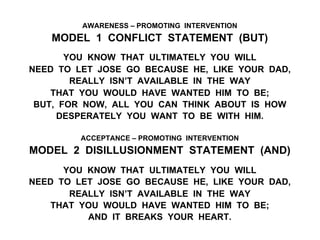
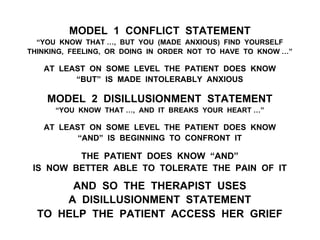
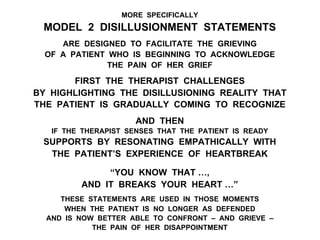
The document outlines an expert perspective on how psychotherapy facilitates healing through an integrative model that encompasses various theories. It emphasizes the importance of achieving optimal stress in the therapeutic process, which allows patients to confront and adapt to emotional challenges and trauma. The book provides a conceptual framework for psychodynamic psychotherapy, illustrating the transformation of maladaptive defenses into healthier adaptive responses via therapeutic action focused on knowledge, experience, and relationship.