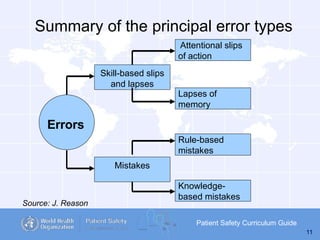
The document serves as a curriculum guide on patient safety, emphasizing the importance of learning from errors to enhance healthcare outcomes. It covers key concepts related to error types, incident reporting, cultural influence in healthcare, and strategies for personal and organizational error reduction. The document advocates for structured approaches like root cause analysis to systematically address and prevent errors in healthcare settings.