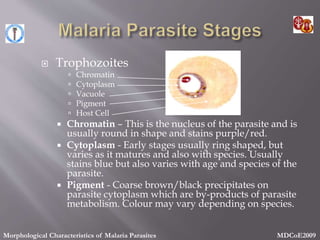
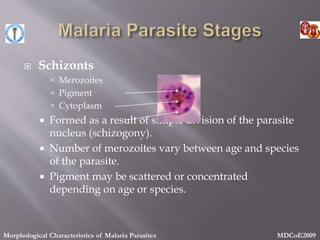
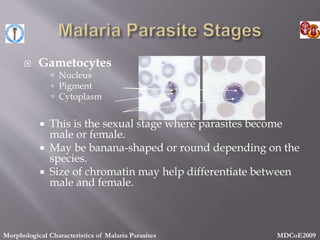
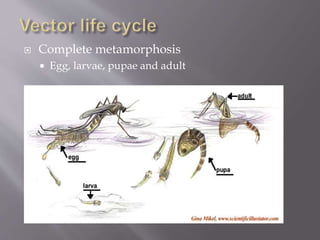
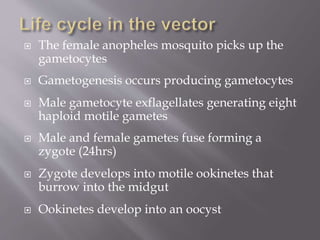
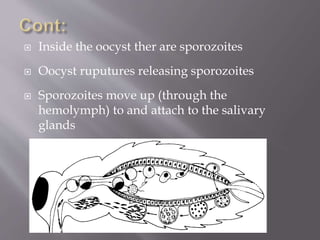
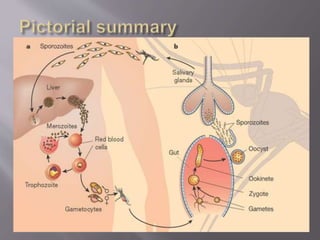
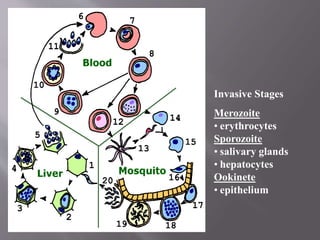
This document discusses malaria transmission and the life cycles of the malaria parasite and mosquito vector. It notes that malaria is transmitted between humans and mosquitoes, with the parasite undergoing development stages in both the liver and blood of humans, and in the gut and salivary glands of mosquitoes. The mosquito life cycle and factors influencing transmission patterns are also summarized.

































![Renal Physiology. [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/renalphysiology-250924082023-9109186b-thumbnail.jpg?width=640&height=640&fit=bounds)






![learning_theories_(skinner_operant_conditioning)[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/learningtheoriesskinneroperantconditioning1-240115075324-0569245b-thumbnail.jpg?width=640&height=640&fit=bounds)














![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














