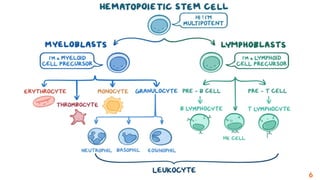
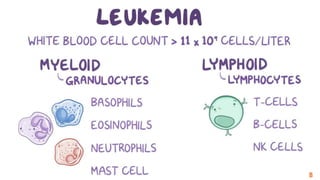
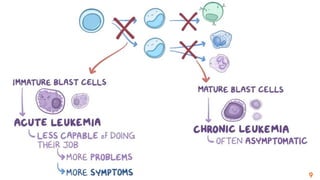
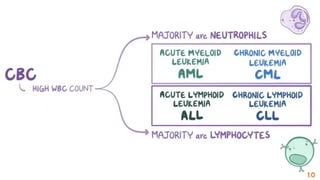
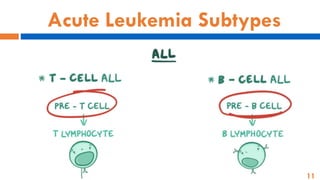
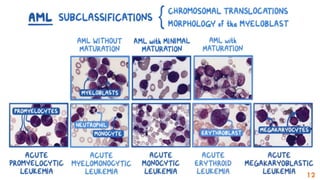
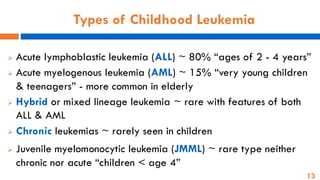
The document provides an overview of childhood leukemia, detailing its types, symptoms, diagnosis, and treatment options. It emphasizes that leukemia is a cancer originating from progenitor cells in the bone marrow, with various subtypes like acute lymphoblastic leukemia and acute myelogenous leukemia being the most common. The treatment approach includes chemotherapy, radiation, and bone marrow transplantation, with stages focusing on inducing remission and maintaining a leukemia-free state.



![Determined based on:
➢ Child's age, overall health, and medical history
➢ Type of leukemia & certain chromosomal changes
➢ Extent of the disease
➢ Child's tolerance for certain medications
➢ Physician’s opinion or preference
[Patient’s Risk Classification]
Treatment](https://image.slidesharecdn.com/leukemiainchildren-3me-241213185915-a776d82a/85/Leukemia-in-children-3-me-pdffffffffffff-26-320.jpg)


















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


