INTRODUCTION
Cancers ofthe hematopoietic system are disorders
that result from the proliferation of malignant cells.
Malignant cells originate in bone marrow, Thymus,
and lymphatic tissue.
Blood cells that originate in bone marrow are called
hematopoietic cells.
4.
Blood cells thatoriginate in lymph are called
lymphoid cells.
Leukemia (Cancer of Bone marrow)
Lymphoma (Cancer of lymphoid tissue)
5.
DEFINITION
Leukaemia isa malignant disease of the blood-forming
organs.
Leukaemia is a malignant progressive disease in which the
bone marrow & other blood-forming organs produce an
increased no. of immature/abnormal leucocytes, which
suppresses the production of normal blood cells, leading to
anaemia & other symptoms.
6.
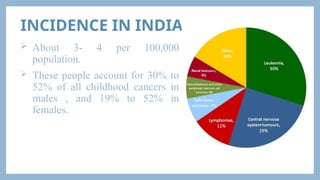
INCIDENCE IN INDIA
About 3- 4 per 100,000
population.
These people account for 30% to
52% of all childhood cancers in
males , and 19% to 52% in
females.
7.
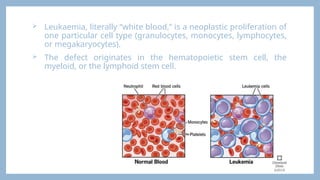
Leukaemia, literally“white blood,” is a neoplastic proliferation of
one particular cell type (granulocytes, monocytes, lymphocytes,
or megakaryocytes).
The defect originates in the hematopoietic stem cell, the
myeloid, or the lymphoid stem cell.
8.
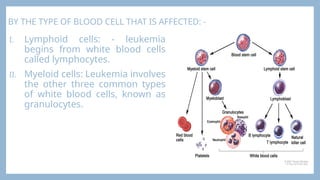
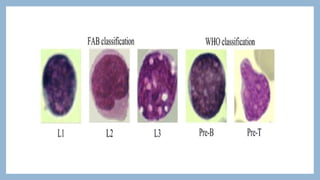
BY THE TYPEOF BLOOD CELL THAT IS AFFECTED: -
I. Lymphoid cells: - leukemia
begins from white blood cells
called lymphocytes.
II. Myeloid cells: Leukemia involves
the other three common types
of white blood cells, known as
granulocytes.
9.
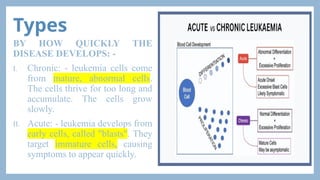
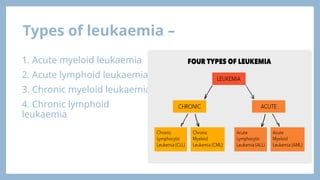
Types
BY HOW QUICKLYTHE
DISEASE DEVELOPS: -
I. Chronic: - leukemia cells come
from mature, abnormal cells.
The cells thrive for too long and
accumulate. The cells grow
slowly.
II. Acute: - leukemia develops from
early cells, called "blasts". They
target immature cells, causing
symptoms to appear quickly.
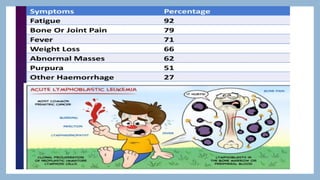
ACUTE LYMPHOBLASTIC LEUKEMIA(ALL)
Acute Lymphoblastic Leukaemia (ALL) results from
uncontrolled proliferation of immature lymphoid cells
(lymphoblasts).
The cell of origin is usually the precursor to the B
lymphocyte in about 75% of cases.
T-lymphocyte ALL occurs in approximately 25% of cases.
ALL is most common in young children.
Boys are affected more often than girls.
The peak incidence is at around 4 years of age.
After age 15 years, ALL becomes relatively uncommon.
Increasing age is associated with reduced survival rates.
12.
ETIOLOGY AND RISKFACTORS
The exact cause is
unknown. Several factors
are associated with
leukemia, including:
SIGN AND SYMPTOMS
Fever and infections caused by
neutropenia.
Weakness and fatigue caused by
anemia.
Bleeding tendencies caused by
thrombocytopenia.
Proliferation of leukemic cells in
organs leads to:
• Pain from an enlarged liver or spleen.
• Gum hyperplasia.
• Bone pain from expansion of marrow.
15.
Problems withlife-threatening infections are common.
Viral infections, such as herpes zoster, can become widely disseminated.
Fever, chills, and other flu-like symptoms.
Weakness and fatigue.
Frequent infections.
Loss of appetite/weight.
Swollen or tender lymph nodes, liver, or spleen.
Tiny red spots (called petechiae) under the skin.
Swollen or bleeding gums.
Sweating, especially at night, and/or Bone or joint pain.
Easy bleeding or bruising.
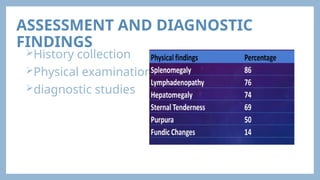
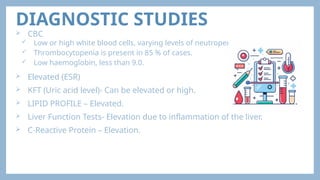
DIAGNOSTIC STUDIES
CBC
Low or high white blood cells, varying levels of neutropenia.
Thrombocytopenia is present in 85 % of cases.
Low haemoglobin, less than 9.0.
Elevated (ESR)
KFT (Uric acid level)- Can be elevated or high.
LIPID PROFILE – Elevated.
Liver Function Tests- Elevation due to inflammation of the liver.
C-Reactive Protein – Elevation.
19.
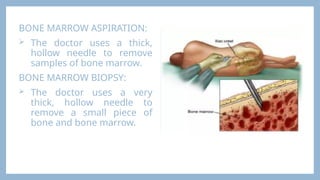
BONE MARROW ASPIRATION:
The doctor uses a thick,
hollow needle to remove
samples of bone marrow.
BONE MARROW BIOPSY:
The doctor uses a very
thick, hollow needle to
remove a small piece of
bone and bone marrow.
21.
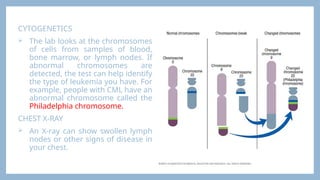
CYTOGENETICS
The lablooks at the chromosomes
of cells from samples of blood,
bone marrow, or lymph nodes. If
abnormal chromosomes are
detected, the test can help identify
the type of leukemia you have. For
example, people with CML have an
abnormal chromosome called the
Philadelphia chromosome.
CHEST X-RAY
An X-ray can show swollen lymph
nodes or other signs of disease in
your chest.
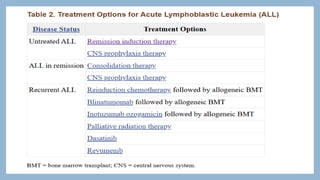
TREATMENT
• Pre-chemotherapy supportivecare
• Chemotherapy
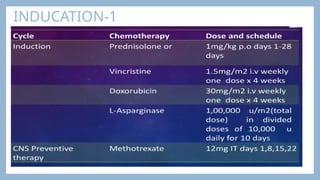
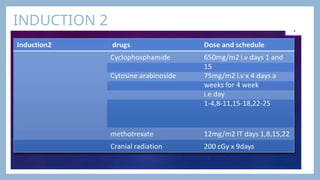
I. Preinduction
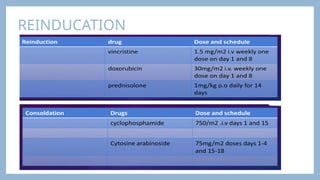
II. Remission induction-phase 1 & 2 Reinduction
III. CNS preventive therapy consolidation
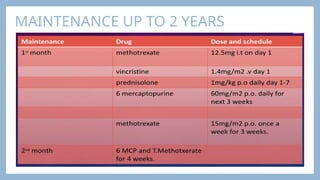
IV. Maintenance therapy
• Allogenic stem cell transplantation
• Newer drugs
• Supportive care
• Treatment of relapse
26.
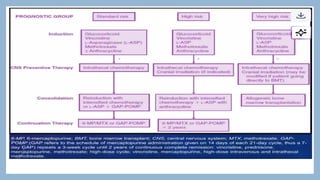
PHASES
Induction therapy:First phase; kills most leukemia cells and
restores normal blood cell production.
Consolidation (post-remission) therapy: Destroys any
leftover leukemia cells.
Maintenance therapy: Prevents leukemia from coming back;
uses lower-dose drugs over years.
CNS (spinal cord) preventive treatment: Given during all
phases; chemo is injected into the spinal fluid to stop the
spread to the brain and spinal cord.
27.
CNS PROPHYLAXIS
Inmost regimens, CNS prophylaxis for patients at lower risk is achieved
with systemic and intrathecal chemotherapy without cranial irradiation.
Children with high-risk features are at an increased risk of CNS relapse
and, historically, have received prophylactic cranial irradiation.
These features include a presenting WBC count of 50,000/μL or greater;
those with WBC counts over 100,000/μL are at particularly high risk of
CNS relapse.
Additional high-risk features that are indications for some treatment
protocols for cranial irradiation are T-cell phenotype, Ph chromosome-
positive ALL, and the presence of t(4;11).
Infants younger than age 12 months with 11q23 abnormalities are at
high risk of CNS relapse, but because of their young age, are usually
treated without cranial irradiation, using intensified systemic and
intrathecal chemotherapy to treat the CNS.
30.
OTHER DRUGS -
Antibiotics to treat bacterial infection.
Anti-viral drugs to treat viral infections.
PPI to treat side effects of chemotherapy.
RADIOTHERAPY
Radiation issometimes used to treat leukaemia that
has spread to the brain and spinal fluid, or to the
testicles.
Radiation to the whole body is often an important
part of treatment before a bone marrow or
peripheral blood stem cell transplant.
BONE MARROW TRANSPLANT
Safely allow treatment of the condition with high
doses of chemotherapy or radiation by replacing or
rescuing damaged bone marrow.
Replace diseased or damaged marrow with new
stem cells.
Provide new stem cells, which can directly help kill
cancer cells.
44.
SPLENECTOMY
If thespleen starts destroying red
blood cells and platelets, it may need to
be removed. This operation is called a
splenectomy.
45.
NURSING MANAGEMENT-Assessment
Obtainhealth history, focusing on fatigue, weight loss, night
sweats, and activity intolerance.
Assess for signs of bleeding & infection.
Evaluate splenomegaly, lymphadenopathy & hepatomegaly.
Difficulty in swallowing, coughing, and rectal pain.
Examine the patient for enlargement of lymph nodes,
hepatosplenomegaly, evidence of bleeding, abnormal
breathing sounds, and skin lesions.
Inspect the patient for signs of infection.
46.
NURSING DIAGNOSIS
1. Acutepain related to tumor growth, infection, or adverse
effects of chemotherapy.
2. Impaired tissue integrity related to high-dose radiation
therapy.
3. Risk for infection includes decreased neutrophils, altered
response to microbial invasion, and presence of
environmental pathogens.
4. Impaired oral mucous membrane related to low platelet
counts and/or effects of pathologic conditions & treatment
as evidenced by oral bleeding.
5. Risk for injury related to low platelet counts & treatment.
47.
Acute pain relatedto tumor growth, infection, or adverse effects of
chemotherapy.
Assess the frequency of pain & administer analgesics on a regular
schedule, as the patient is monitored for adverse effects.
Provide a comfortable position to the patient to promote comfort.
Advise the patient for the use of non-pharmacologic methods, music
therapy, relaxation, distraction & imagery to help manage pain.
Provide a calm environment for the patient to promote physical
comfort.
Provide diversional therapy to the patient to divert the patient from
pain.
Provide psychological support to the patient.
Advise the patient to restrict the activity that generates pain.
48.
Impaired tissue integrityrelated to high-dose radiation
therapy.
Avoid rubbing powders, deodorants, lotions or ointments
(unless prescribed) or application of heat & cold to treated
areas.
Encourage the patient to keep the treated area clean & dry.
Advise the patient to bathe the area gently with tepid water &
mild soap.
Encourage the patient to wear loose-fitting clothes.
Advise the patient to protect skin from overexposure to
sunlight, chlorine & temperature extremes.
49.
Risk for infectionto decreased neutrophils, altered response to microbial
invasion, and presence of environmental pathogens.
Intervention plan:
Inspect the patient for the sign & symptoms of infection e.g. redness etc.
Maintain asepsis for patient at risk.
Instruct the patient to take antibiotics as prescribed by doctor to prevent microbial
resistance.
Teach the patient & family how to avoid infections e.g. about personal hygiene
technique of hand washing, oral care, skin hygiene etc.
Educate the patient to report if there is any presence of signs of infection to the
doctor immediately.
Monitor granulocyte count & WBC count to identify the presence of infection.
Screen all visitors for communicable diseases.
50.
Impaired oral mucousmembrane related to low platelet counts
and/or effects of pathologic conditions & treatment as evidenced by
oral bleeding.
Plan for interventions:
Monitor lips, tongue, mucous membrane, tonsillar fossae & gums for
moisture, color, texture, presence of debris & infection.
Assist the patient to select soft, bland, & non acidic foods to decrease
irritation of oral mucosa.
Advise the patient to use soft toothbrush for removal of dental debris.
Instruct the patient to perform oral hygiene after eating & as often as
needed to avoid breakdown of oral mucosa.
Advise the patient to avoid the use of lemon-glycerine swabs to
prevent excessive drying of the mucosa.
51.
Risk for injuryrelated to low platelet counts & treatment.
Intervention plan:
Monitor the patient for the signs & symptoms of persistent bleeding to detect
internal bleeding.
Monitor for the prothrombin time (PT), partial thromboplastin time (PTT),
fibrinogen, fibrin degradation products & platelet count to determine bleeding
risk.
Protect the patient from trauma that may cause bleeding to reduce tissue
trauma & subsequent bleeding in tissue.
Administer blood products (e.g., platelets, fresh frozen plasma) to replace
coagulation factor.
Teach the patient to avoid aspirin or other anticoagulants to prevent additional
bleeding risk.
Educate the patient about the harm of injury to the patient as well as to family
members.



































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



