Downloaded 20 times
![ity is typically made after confirmation of normal
ovarian reserve and ovulatory markers, tubal pa-
tency, and partner semen analysis.2 Controlled
ovarian stimulation (COS) is generally considered
a first-line treatment in patients with unexplained
infertility, and several agents with different modes
of action are commonly employed.
Two oral agents that have been widely used for
COS are the selective estrogen receptor modulator
clomiphene citrate (CC) and the third generation
aromatase nonsteroidal inhibitor (AI) letrozole
(LET). CC clomiphene citrate has been widely used
worldwide, and it is the first choice in normo
gonadotropic oligo/amenorrheic infertility (World
Health Organization [WHO] group 2).3 CC is a non-
steroidal triphenylethylene derivative that exhibits
both estrogenic agonist and antagonist properties,
although its estrogenic agonist properties man-
ifest only when endogenous estrogen levels are
extremely low.4 CC acts by binding to estrogen
receptors (ERs) in the hypothalamus, causing a
perceived drop in circulating estrogens, which
increases gonadotropin secretion by the pituitary
and subsequent ovulation.5 Various adverse ef-
fects have been described, mainly secondary to its
antiestrogenic action, including hot flashes, pre
menstrual syndrome–like symptoms, suboptimal
endometrial thickness, and decreased cervical
mucus production, all of which are also associ-
ated with reducing pregnancy rates. Lastly, CC is
more likely to produce a multifollicular response,
potentially increasing the multiple pregnancy
rates.6,7 Laterally with CC treatment, intrauter-
ine insemination (IUI) has been widely used to
circumvent the poor cervical mucus production,
and human chorionic gonadotropin (hCG) trigger
is typically employed in those cycles in an effort
to appropriately time insemination procedures.8,9
Nevertheless, although the routine use of timed
IUI has been shown to be beneficial by numerous
studies, overall outcomes remain ambiguous, with
many previous reports not supporting its use.10-15
Letrozole is a potent, reversible AI approved by
the FDA as a chemotherapeutic agent in postmeno-
pausal women with metastatic cancer16; it has been
used in reproductive medicine since 2001.17 When
aromatization of androgens is inhibited, the re-
sulting reduction of circulating estrogens pro-
motes the growth of ovarian follicles through the
increased secretion of follicle-stimulating hormone
(FSH), yielding a transient intraovarian androgen
ic environment. This appears to increase follicular
sensitivity to FSH without antagonizing ERs, thus
avoiding an antiestrogenic affection on the endo
metrial lining.5 Although LET stimulation can re
sult in some side effects such as hot flashes, muscle
aches, and gastrointestinal disturbances,19 the side
effect profile is typically well tolerated. Further-
more, LET appears to cause fewer congenital ab-
normalities in comparison to CC.18 Although both
CC and LET have both been widely utilized for
COS in IUI protocols, the choice of agent is largely
a matter of physician discretion, and the current
opinion favors LET to increase PRs.20
To date, several prospective, randomized stud
ies and metaanalyses comparing these agents have
contributed to our current knowledge base.5-7 LET
has appeared to be just as safe and effective as CC.
However, small sample sizes (<100 patients) and
conflicting studies have left physicians indefinite
as to the significance and applicability of prior
results. Recently, LET has been advocated as the
optimal agent for ovulation induction due to an
observed decrease in the frequency of its side
effects, thus leading to an increasingly favorable
attitude in its use for standard care in many cen-
ters. We previously conducted a retrospective anal-
ysis that compared LET versus CC efficacy com-
bined with IUI in patients with unexplained infer-
tility and demonstrated a trend towards higher PRs
with LET usage.21
Given the fact that LET is associated with min-
imal antiestrogenic effects, we postulated that the
use of IUI would not enhance the PR of LET cycles.
In order to test this hypothesis, we compared re-
productive outcomes in patients with unexplained
infertility who underwent a LET cycle with timed
sexual intercourse (IC) to those who underwent a
CC cycle with timed IUI.
Materials and Methods
Patient Information
This observational, retrospective cohort study was
performed at an academic, private fertility practice.
We reviewed the electronic medical records of all
patients undergoing treatment with CC or LET
from January 2010 to June 2014. The choice of COS
protocol was determined by the treating physician.
Patients <40 years of age diagnosed with unex-
plained infertility (normal ovarian reserve screen-
ing [day 3 FSH ≤12.5 mUI/mL, day 3 estradiol ≤80
pg/mL, and AMH ≥1 ng/mL]) with partners having
normal semen analysis according to WHO param-
eters22 were included in the study. Only cycles
2 The Journal of Reproductive Medicine®](https://image.slidesharecdn.com/232214ee-0fa7-43fc-b7e0-20b3b16057f5-161229220500/75/LETROZOLE-WITH-TIMED-INTERCOURSE-VERSUS-CLOMIPHENE-CITRATE-WITH-IUI-2-2048.jpg)
![and a trend toward pregnancy rates that were high-
er than those found in patients undergoing CC
and IUI. We suggest that physicians consider LET
and timed IC rather than CC and IUI for the treat-
ment of unexplained infertility.
References
1. Practice Committee of the American Society for Reproductive Med-
icine: Effectiveness and treatment for unexplained infertility. Fertil
Steril 2006;86:1001
2. Ray A, Shah A, Gudi A, et al: Unexplained infertility: An update and
review of practice. Reprod Biomed Online 2012;24:591-602
3. Seli E, Arici A: Ovulation induction with clomiphene citrate. In
UpToDate. Edited by RL Barbieri. Wolters Kluwer Health/UpTo-
Date,Inc.Availableathttp://www.uptodate.com/contents/ovulation-
induction-with-clomiphene-citrate. Accessed ____________
4. Practice Committee of the American Society for Reproductive Med-
icine: Use of clomiphene citrate in infertile women: A committee
opinion. Fertil Steril 2013;100:341-348
5. Requena A, Herrero J, Landeras J, et al: Use of letrozole in assisted
reproduction: A systematic review and meta-analysis. Hum Reprod
Update 2008;14:571-582
6. Polyzos NP, Tzioras S, Mauri D, et al: Treatment of unexplained in
fertility with aromatase inhibitors or clomiphene citrate: A systematic
review and meta-analysis. Obstet Gynecol Survey 2008;63:472-479
7. He D, Jiang F: Meta-analysis of letrozole versus clomiphene citrate in
PCOS. Reprod Biomed Online 2011;23:91-96
8. Zreik TG, García-Velasco JA, Habboosh MS, et al: Prospective, ran-
domized, crossover study to evaluate the benefit of human chorionic
gonadotropin-timed versus urinary luteinizing hormone-timed in-
trauterine inseminations in clomiphene citrate-stimulated treatment
cycles. Fertil Steril 1999;71:1070-1074
9. Kosmas IP, Tatsioni A, Fatemi HM, et al: Human chorionic gonad-
otropin administration vs. luteinizing monitoring for intrauterine
insemination timing, after administration of clomiphene citrate: A
meta-analysis. Fertil Steril 2007;87:607-612
10. Veltman-Verhulst SM, Cohlen BJ, Hughes E, et al: Intrauterine insemi-
nation for unexplained subfertility. Cochrane Database Syst Rev 2012;
(9):CD001838
11. Cohlen BJ, Vandekerckhove P, te Velde ER, et al: Timed intercourse
versus intrauterine insemination with or without ovarian hyperstim-
ulation for subfertility in men. Cochrane Database Syst Rev 2000;(2):
CD000360
12. Helmerhorst FM, van Vliet HA, Gornas T, et al: IUI versus timed IC
for cervical hostility in subfertile patients. Obstet Gynecol Surv 2006;
61:402-414; quiz 423
13. Barros-Delgadillo JC, Martinez-Barrios E, Moreno-Aburto C, et al:
[Intrauterine insemination versus programmed intercourse in cycles
of controlled ovaric hyperstimulation]. [Article in Spanish] Ginecol
Obstet Mex 2008;76:18-31
14. Abu Hashim H, Ombar O, Abd Elaal I: Intrauterine insemination
versus timed intercourse with clomiphene citrate in polycystic ovary
syndrome: A randomized controlled trial. Acta Obstet Gynecol Scand
2011;90:344-350
15. Check JH, Liss J, Bollendorf A: Intrauterine insemination (IUI) does
not improve pregnancy rates in infertile couples where semen param-
eters are normal and postcoital tests are adequate. Clin Exp Obstet
Gynecol 2013;40:33-34
16. Lamb HM, Adkins JC: Letrozole: A review of its use in postmeno-
pausal women with advanced breast cancer. Drugs 1998;56:1125-1140
17. Fisher SA, Reid RL, Van Vugt DA, et al: A randomized double-blind
comparison of the effects of clomiphene citrate and the aromatase
inhibitor letrozole on ovulatory function in normal women. Fertil
Steril 2002;78:280-285
18. Casper RF, Mohamed FM: Historical perspective of aromatase in-
hibitors for ovulation induction. Fertil Steril 2012;98:1352-1355
19. Tulandi T, Martin J, Al-Fadhli R, et al: Congenital malformations
among 911 newborns conceived after infertility treatment with letro-
zole or clomiphene citrate. Fertil Steril 2006;85:1761-1765
20. Palatnik A, Strawn E, Szabo A, et al: What is the optimal follicular size
before triggering ovulation in intrauterine insemination cycles with
clomiphene citrate or letrozole? An analysis of 988 cycles. Fertil Steril
2012;97:1089-1094.e1-3
21. Mukherjee T, Whitehouse M, Lee JA, et al: The efficacy of insemi-
nation in letrozole versus clomiphene citrate treatment cycles. Fertil
Steril ____;100:Suppl S261-000
22. Cooper TG, Noonan E, von Eckardstein S, et al: World Health Or-
ganization reference values for human semen characteristics. Hum
Reprod Update 2010;16:231-245
23. Kar S: Current evidence supporting “letrozole” for ovulation induc-
tion. Hum Reprod Sci 2013;6:93-98
24. Bhattacharya S, Harrild K, Mollison J, et al: Clomiphene citrate or
unstimulated intrauterine insemination compared with expectant
management for unexplained infertility: Pragmatic randomised con-
trolled trial. BMJ 2008;337:a716
6 The Journal of Reproductive Medicine®](https://image.slidesharecdn.com/232214ee-0fa7-43fc-b7e0-20b3b16057f5-161229220500/75/LETROZOLE-WITH-TIMED-INTERCOURSE-VERSUS-CLOMIPHENE-CITRATE-WITH-IUI-6-2048.jpg)

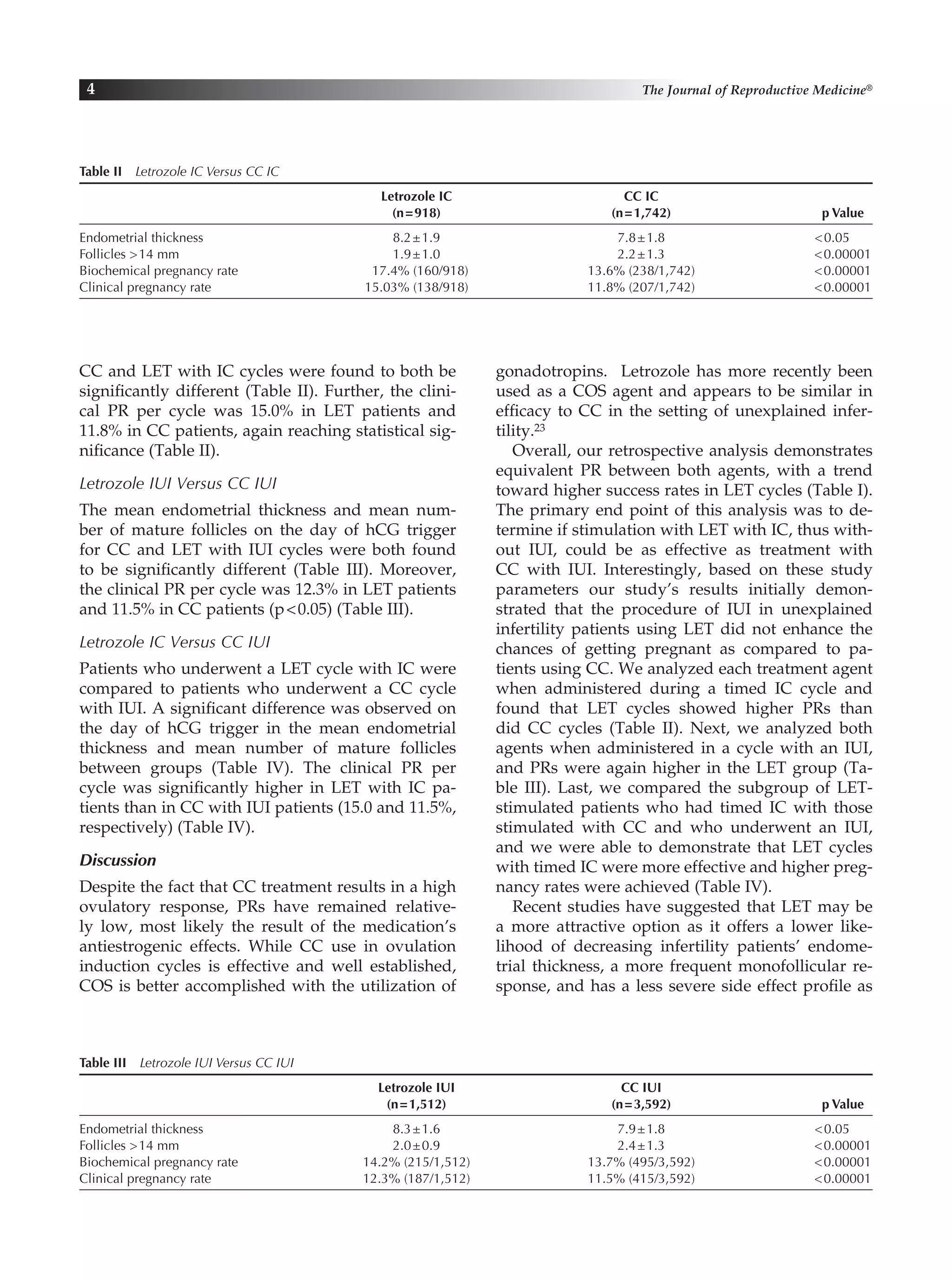
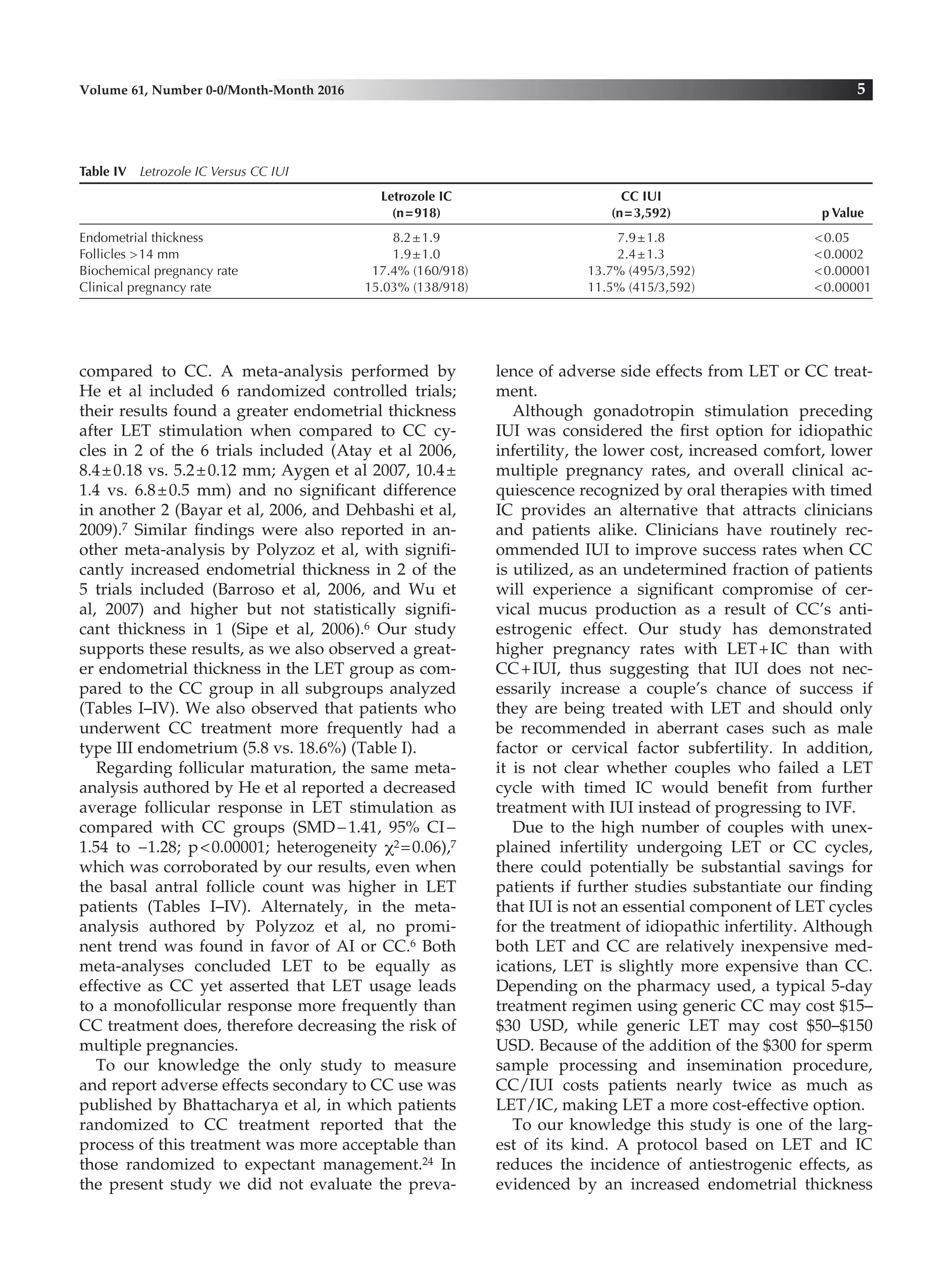
This study compared pregnancy outcomes in 7,764 patients with unexplained infertility who underwent controlled ovarian stimulation (COS) with either letrozole (LET) and timed intercourse (IC) or clomiphene citrate (CC) and intrauterine insemination (IUI). Clinical pregnancy rates were significantly higher in the LET-IC group compared to the CC-IUI group (15.0% vs 11.8% for IC, 12.3% vs 11.5% for IUI). Endometrial thickness and follicular response were also higher in the LET group. The study concluded that unexplained infertility patients have better pregnancy outcomes with LET stimulation and timed IC compared to CC stimulation and timed ICI

































































