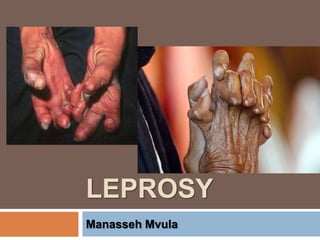
2. Definition
Leprosy (Hansen’s disease) is a chronic
infectious disease caused by the acid-fast,
rod-shaped bacillus Mycobacterium leprae
The disease mainly affects the skin, the
peripheral nerves, mucosal surfaces of the
upper respiratory tract and the eyes
Can occur at all ages ranging from early
infancy to very old age
3. Properties of M. leprae
Acid fast rod-shaped bacillus
Grow very slowly taking up to 20 years to
develop signs of the infection
Obligate intracellular pathogen – lacks
several genes needed for independent
survival
Incubation period: 6 months - 40 years or
longer (4 years for tuberculoid leprosy (TT)
and 10 years for lepromatous leprosy (LL).
4. Prevalence
Race
occurs in all races
Leprosy is endemic in Asia, Africa, the Pacific
basin
Sex
Leprosy is generally more common in males than
in females, with a male-to-female ratio of 2:1.
Age
can occur at any age, though very rare in infants
5. Transmission
The exact mechanism of transmission of
leprosy is not known
The principle means of transmission is by
aerosol spread from infected nasal
secretions to exposed nasal and oral
mucosa
It is believed that leprosy is transmitted by
Prolonged, and close contact with
someone with untreated leprosy over
many months
7. Tuberculoid Leprosy
Skin lesions are single or few
Sharply demarcated
Anesthetic or hyperesthetic and
bilaterally symmetrical
Peripheral nerve involvement tends
to be severe
8. Lepromatous Leprosy
Nodules, papules, macules
Diffused infiltration are bilaterally
symmetrical and usually numerous
and extensive
Involvement of the nasal mucosa may
lead to crusting, obstructed breathing
and epistaxis
Ocular involvement leads to iritis and
keratitis
9. Cont’d
Another classification (WHO)
depends on the number of
lesions and bacterial index (BI)
Paucibacillary
Multibacillary
11. Paucibacillary
Has fewer than 5 lesions
No bacilli on smear testing
Has two other classes
Indeterminate Leprosy (IL)
Tuberculoid Leprosy (TT)
12. Cont’d
Indeterminate Leprosy (IL)
This early form causes one to a few
hypopigmentated or sometimes erythematous
macules
Sensory loss is unusual
Tuberculoid Leprosy (TT)
Skin lesions are few
One erythematous large plaque is usually
present, with well-defined borders that are
elevated and that slope down into an atrophic
center
13. Multibacillary
Has Five or more lesions with or
without bacilli
Classes include:
Borderline
Lepromatous
14. Cont’d
Borderline Tuberculoid leprosy (BT)
Lesions in this form are similar to those in the
tuberculoid form, but they are smaller and
more numerous.
Borderline borderline leprosy (BB)
Cutaneous lesions consist of numerous, red,
irregularly shaped plaques that are less well
defined than those in the tuberculoid type.
15. Cont’d
Borderline lepromatous leprosy (BL)
Lesions are numerous and consist of
macules, papules, plaques, and nodules
Lepromatous Leprosy (LL)
Early cutaneous lesions consist mainly of
pale macules
Late infiltrations are present with numerous
bacilli Macular lesions are small, diffuse, and
symmetric
16. Pathophysiology
In general, leprosy affects the skin,
peripheral nerves, and eyes
Systemic symptoms may occur
Specific symptoms vary with the
severity of the disease
17. Cont’d
Leprosy can manifest in different
forms, depending on the host
response to the organism
Individuals who mount cellular
immune response to M. leprae have
the tuberculoid form of the disease
that usually involves the skin and
peripheral nerves
18. Cont’d
Individuals with minimal cellular immune
response have the lepromatous form of
the disease, which is characterized by
extensive skin involvement
The strength of the host’s immune system
influences the clinical form of the disease
19. Cont’d
A strong cell-mediated immunity and a weak
humoral response results in mild forms of
disease, with a few well-defined nerves involved
and lower bacterial loads
A strong humoral response but relatively absent
cell-mediated immunity results in LL, with
widespread lesions, extensive skin and nerve
involvement, and high bacterial loads
The organism grows best at 27-30°C; therefore,
skin lesions tend to develop in the cooler areas
of the body, with sparing of the groin, axilla, and
20. Signs and Symptoms
Prodromal: Pts have a history of
numbness first, sometimes years before
the skin lesions appear
Patient cannot sense extremes of hot or
cold
The next sensation lost is light touch, then
pain, and finally deep pressure.
These losses are especially apparent in the
hands and feet; therefore, the chief complaint
may be a burn or ulcer in an anesthetic
extremity
21. 21
Signs and Symptoms
Tuberculoid leprosy
Asymetrical
Localised circular hypopigmented
patches.
Hypoasthetic (sensation will be
reduced or no sensation)
Thickening of peripheral nerves.e.g
alna nerve
22. 22
Signs and Symptoms
Lepromatous leprosy
Insideous onset
Has wide spread symetrical
hypopigmented patches.
Mucosal thickening and becomes
yellow discolouration, particulary the
nasal mucosal.
Conjuctivitis which may progress to
blindness.
Autoamputation (digits; fingers fall
off)
Colapse of the nasal bridge inwards
23. 23
Investigations
History
Physical examination
Lepromin test
+ve in tuberculoid
-ve in lepromatous
Skin smear for AAFB
+ve lepromatous
-ve in tuberculoid
Biopsy of skin lesions
Caseating lesions in tuberculoid
24. 24
Treatment
Medical
Dapsone 250mg twice weekly or daily
Rifampicin 600mg
Steroid- prednisolone
Supportive
Orthopaedic treatment for deformities.
Psychological treatment
25. 25
NURSING CARE OF A PATIENT WITH
LEPROSY
Admission
Patients are admitted to a
hospital called leprosarium in
the initial phase
To stabilise on treatment
For monitoring of side effects of
drugs
For constructive surgery if
26. 26
NURSING CARE OF A PATIENT WITH
LEPROSY
Psychological care
Patient will be worried about self-
esteem and that they will be treated
as an outcast.
Involve the family members, educate
them on the disease and their attitude
which will affect the patient on self
image.
Allow patient to get involved in family
affairs.
27. Cont’d
Family should not isolate patient.
Explain that when the patient is on treatment,
there is no possibility of contracting infection.
Patient needs to be kept busy.
They can be taught simple skills e.g gardening,
cooking, sewing, making mats.
These measures prevent boredom and lessens
emotional problems.
It also gives an art which they can use to earn
an income.
28. 28
NURSING CARE OF A PATIENT WITH
LEPROSY
Nutrition
Build and maintain the nutritional
status of the patient to help build
patient’s resistance to the
disease.
Patient requires a high nutritious
diet with iron and vitamin
supplements for tissue repair as
well as for maintenance of normal
haemoglobin levels.
29. 29
NURSING CARE OF A PATIENT WITH
LEPROSY
Observations
Routine vital sign check
Keep on monitoring the degree of loss
of sensation.
Observe for drug reaction, e.g skin
reaction like rashes, psychosis etc.
Protect the patient from injury i.e
burns, broken bottles because patient
wont feel any pain when hurt.
30. 30
NURSING CARE OF A PATIENT WITH
LEPROSY
I.E.C
Teach the patient about this
condition in simple terms.
Teach them about the importance
of drug administration to achieve
effectiveness and control
progress of disease.
Teach them on food and personal
hygiene.
31. 31
NURSING CARE OF A PATIENT WITH
LEPROSY
Tell patient that the affected parts
like the legs, hands should be
kept dry and clean all the time to
prevent infection.
Teach them to wear protective
foot wear to prevent injury.
Teach them on the importance of
plastic surgery in order to correct
deformity.
32. 32
REHABILITATION IN LEPROSY
Measures to regain usefulness of
an individual and also making the
patient psychologically
dependence are done.
There are 3 types of
rehabilitation:
Physical
Occupational
emotional
33. 33
REHABILITATION IN LEPROSY
Physical rehabilitation
Prevention
Help patient to get over physical
disabilities of leprosy e.g physical
deformities and blindness.
To prevent disability there is need for
early diagnosis, early treatment and
the need to recognise early reactions
of nails and eyes and treat them
promptly.
34. 34
REHABILITATION IN LEPROSY
Management of disability
Control the ulcerations
Avoid destruction of extremities
Teach patient on the care of
anaesthetised part.
Make him be aware of the
abnormality; he should have
protective foot wear.
35. 35
REHABILITATION IN LEPROSY
Restrict the use of the anaesthetised part.
Advise patient to protect the hands by using
gloves.
Dead and coloured tissues can be removed
in the hospital.
Skin grafting should be done on ulcerations,
reserving paralysed muscles and those not
in use to prevent atrophy.
36. 36
REHABILITATION IN LEPROSY
Physiotherapy
Aims
To prevent contractures
To retain full range of motion
To prevent muscular atrophy
To prevent overstretching of paralysed
muscles
To assist in gaining normal muscle power
37. 37
REHABILITATION IN LEPROSY
Implementation
Do passive exercises
Massage
Electrical stimulation
splinting of immobile parts
38. 38
REHABILITATION IN LEPROSY
Reconstructive surgery
Indications
Functional purposes
Entropion inversion of eyelid so that they rub against
the eyeball.
Facial nerve palsy
Hand paralysis
Foot drop
Amputation
Claw toes
39. 39
REHABILITATION IN LEPROSY
Cosmetic reasons
Replacement of eyebrows
Nasal collapse
Sagging face or earlobes
Gynaecomastia
Prosthetic reasons
Artificial leg or amputation
40. 40
REHABILITATION IN LEPROSY
Emotional (social & physical) rehabilitation
Socially patient is fearful, anxious and feels
rejected and he/she might think that he/she
can transmit infection to the family.
Reasure patient
Talk to the family and community on the
importance of accepting the patient.
Explain on the condition and how they will
protect the patient.
41. 41
REHABILITATION IN LEPROSY
Occupational (vocational ) rehabilitation
This varies according to peoples’ attitudes,
opportunities and the availability of farm land.
Control of Leprosy
Early diagnosis and treatment of infectious
cases.
Out patient care should be within reach
42. 42
CONTROL OF LEPROSY
Case finding and surveys
IEC to infected cases and community
Immunisation for those at risk i.e babies
in infected families.
Children below 10 years with infected
parents are put on prophylactic treatment.