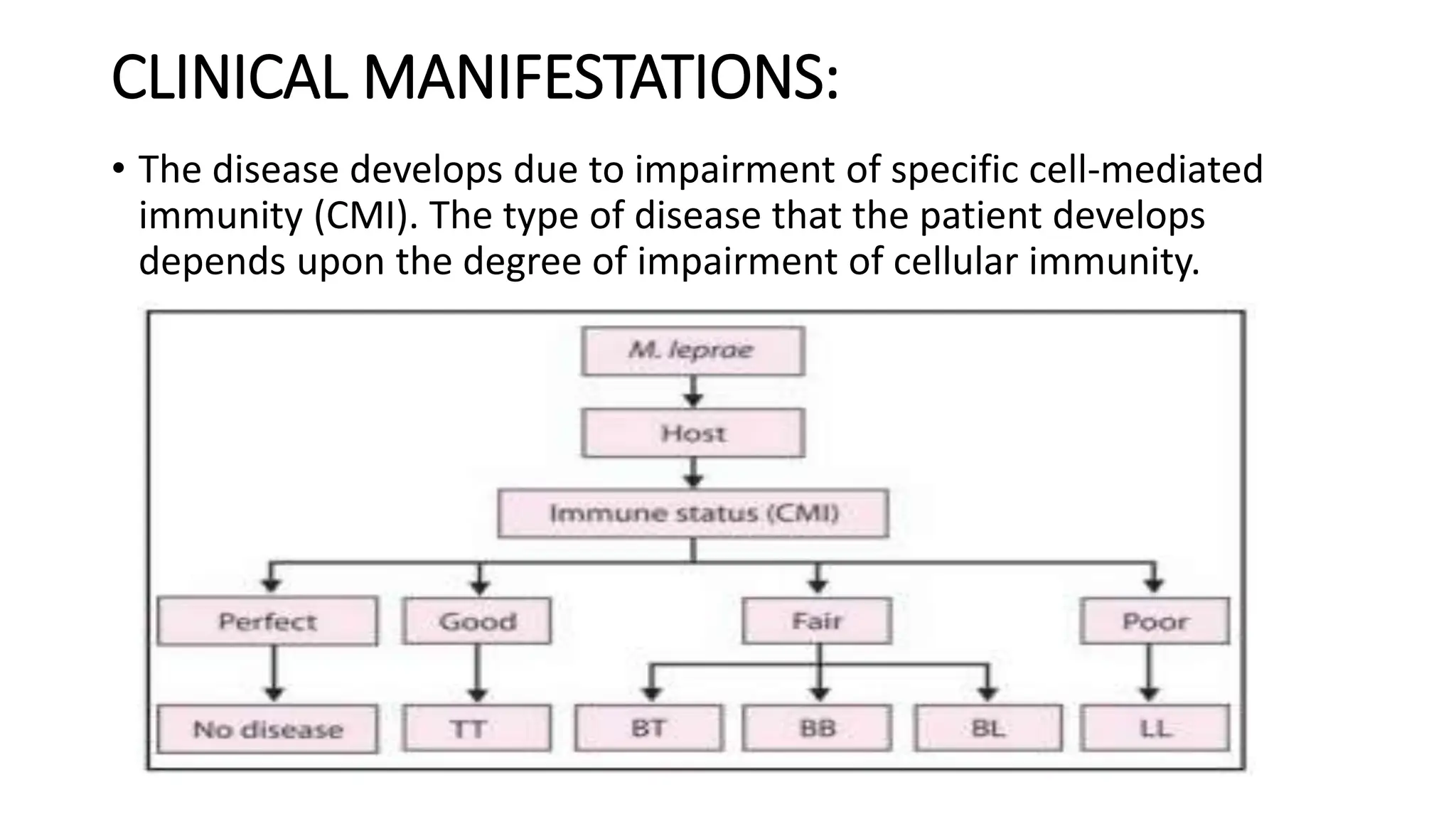
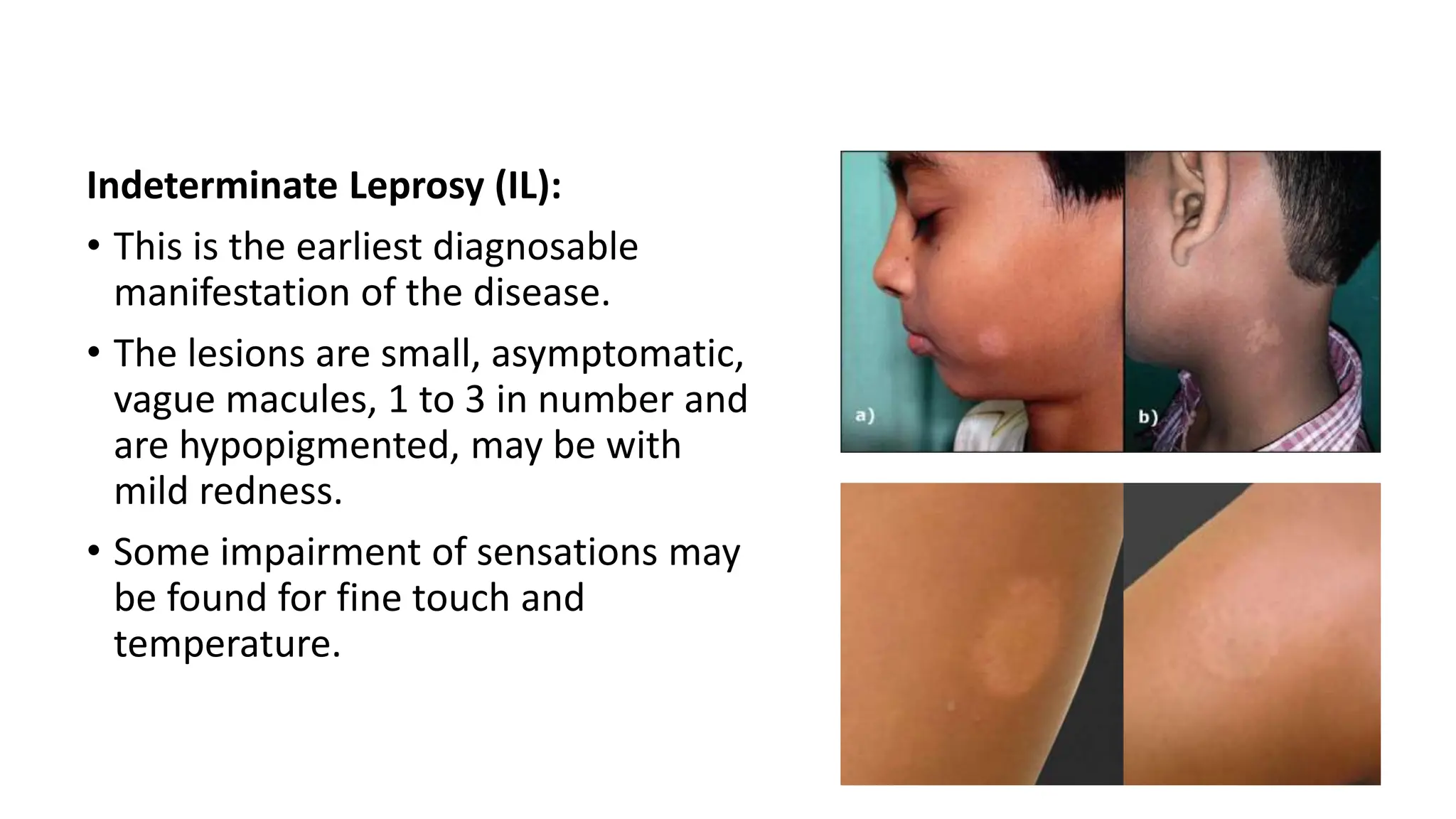
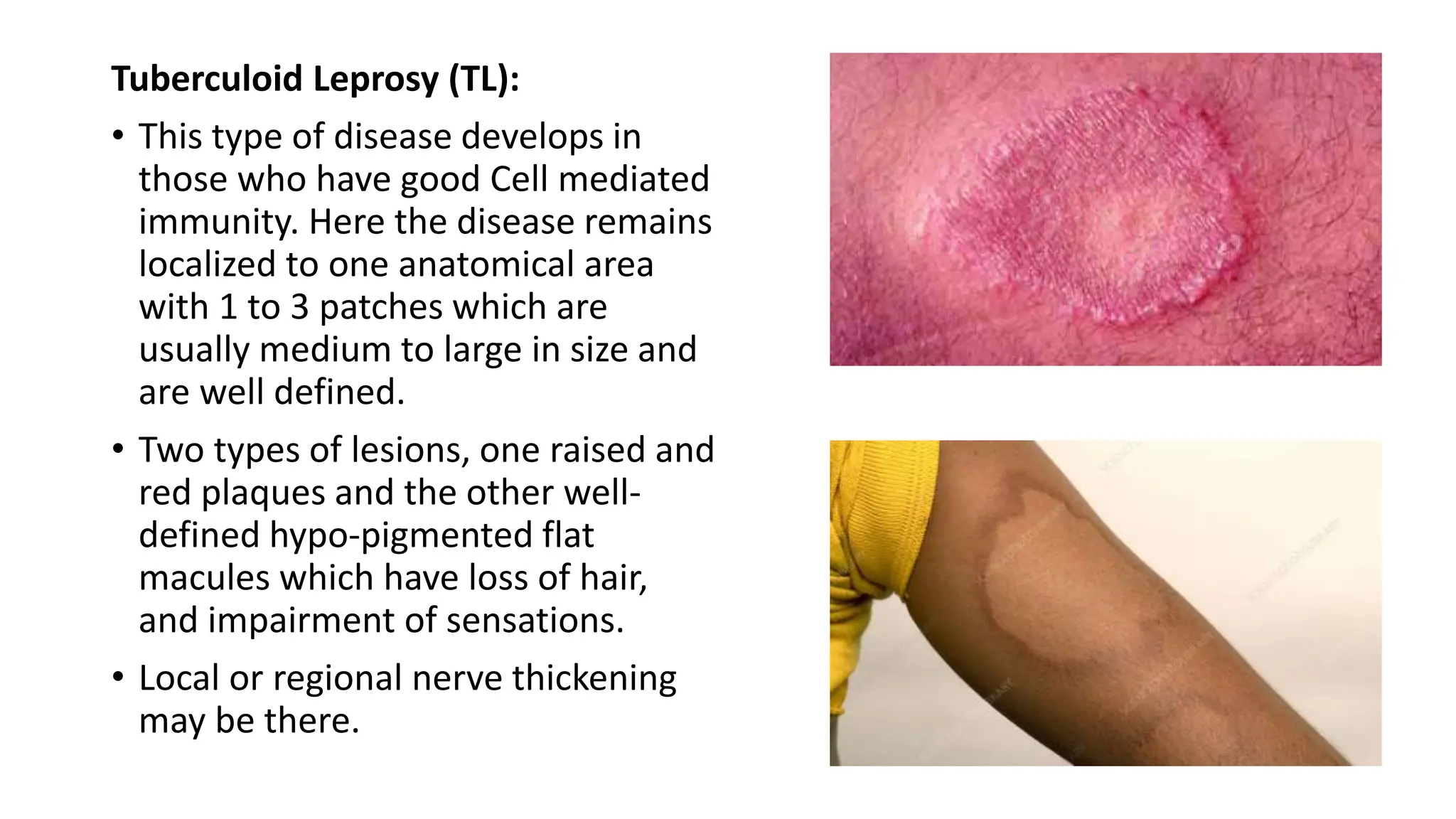
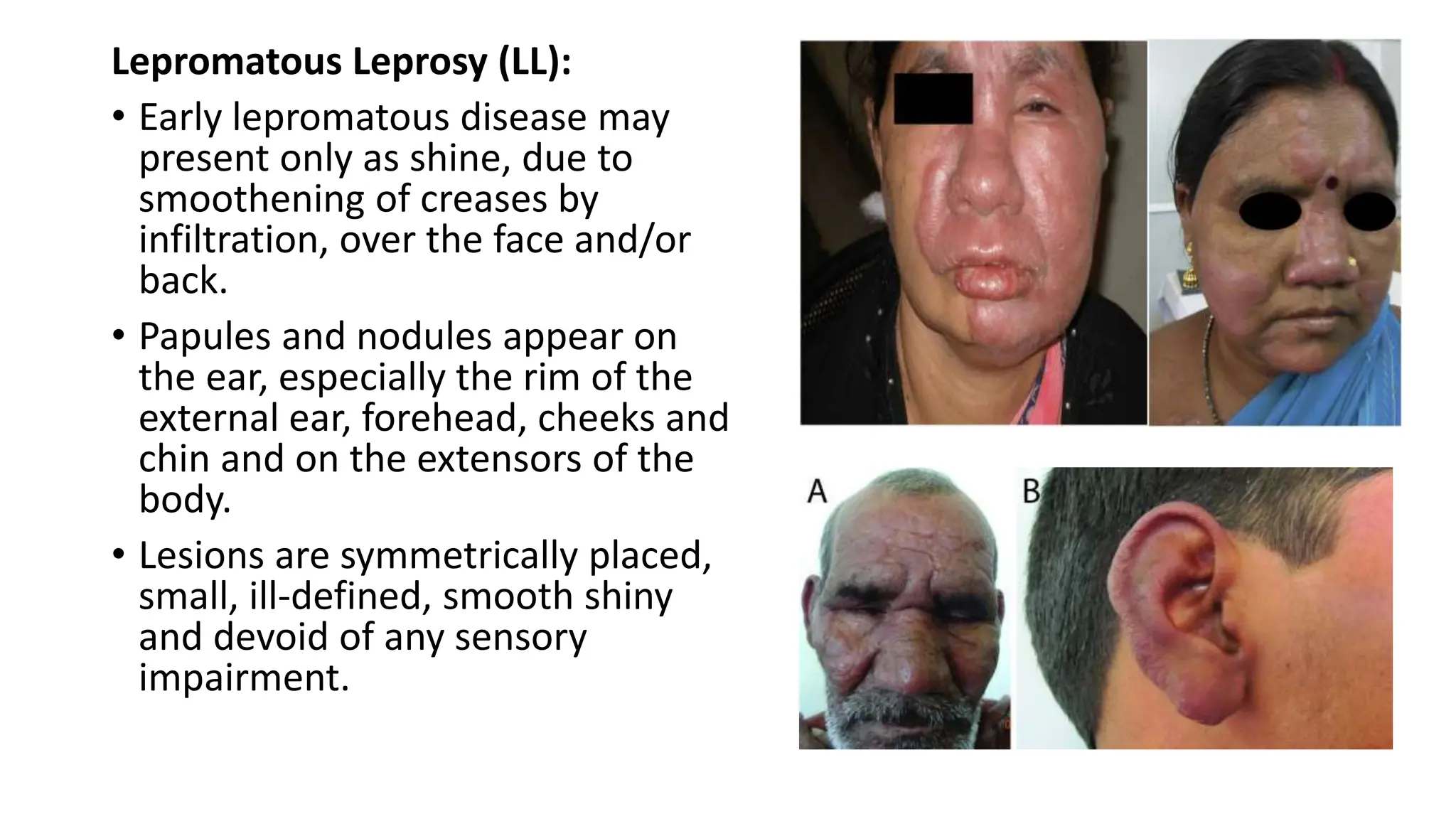
This document is a presentation about leprosy (Hansen’s disease), a chronic infectious disease caused by Mycobacterium leprae, primarily affecting the skin and peripheral nerves. It discusses epidemiology, transmission, clinical manifestations (including types of leprosy), laboratory investigations, and potential homeopathic treatments. The various forms of leprosy depend on the degree of impairment of cellular immunity, with specific characteristics outlined for each type.