Introduction to shock
Possiblecauses of shock
Pre-shock symptoms
Sign and symptoms
Assessment of Shock Patient
Generalized Treatment
Types of shock
Management of each shock type
accordingly
Monitoring and care to the shock
patient
Topic
Outlines
3.
Acute circulatoryfailure.
Decreased organs perfusion.
Inadequate oxygen delivery.
End organ dysfunction.
Actually it is the imbalance between demand and supply of oxygen.
Inability to utilize oxygen
A temporary stage of unconsciousness.
Shock
4.
Failure ofoxygen delivery system
◦ Hypoxia
◦ Oxygen deficient environment
i.e. high altitude.
Injury to the lungs/ Lung disease/
unable to transform oxygen into
the blood.
◦ Pneumonia
◦ CHF
◦ Traumatized lungs
◦ Pulmonary embolism
◦ Pulmonary edema
◦ Hemo/hydro/pneumothorax
◦ Respiratory arrest
Burns
Diarrhea/vomiting (persistent)
Spinal injuries (neurogenic)
Heart related problems
◦ CHF
◦ MI
◦ Heart attack/cardiac arrest
◦ Arrhythmias
◦ Pericarditis/endocarditis
◦ Pericardial effusion
◦ CAD
RBCs related
◦ Anemia
◦ Bleeding disorders
◦ Hemolysis
Body fluids (dehydration)
Hypotension due to
vasodilation or any other
causes.
Possible
Causes of
Shock
5.
Rapid butshallow breathing
Feeling to get fainted
Dizziness starts
Blacking out of eye
Nausea
Feeling of General weakness
Facial flushing
Pre-shock
Symptoms
6.
Low Bp
Tachycardia
(compensatory)
Rapid but shallow
breathing persists
Cold and clammy skin
Rapid but weak pulse
Dizziness/fainting
General weakness
Type dependent sign
and symptoms
◦ Anxiety or agitation
◦ Seizures
◦ Confusion/
unresponsiveness
◦ Low or no urine
output
◦ Peripheral cyanosis
◦ Sweating
◦ Chest pain.
Sign and
Symptoms
7.
ABC Protocol
◦Airway
◦ Breathing
◦ Circulation
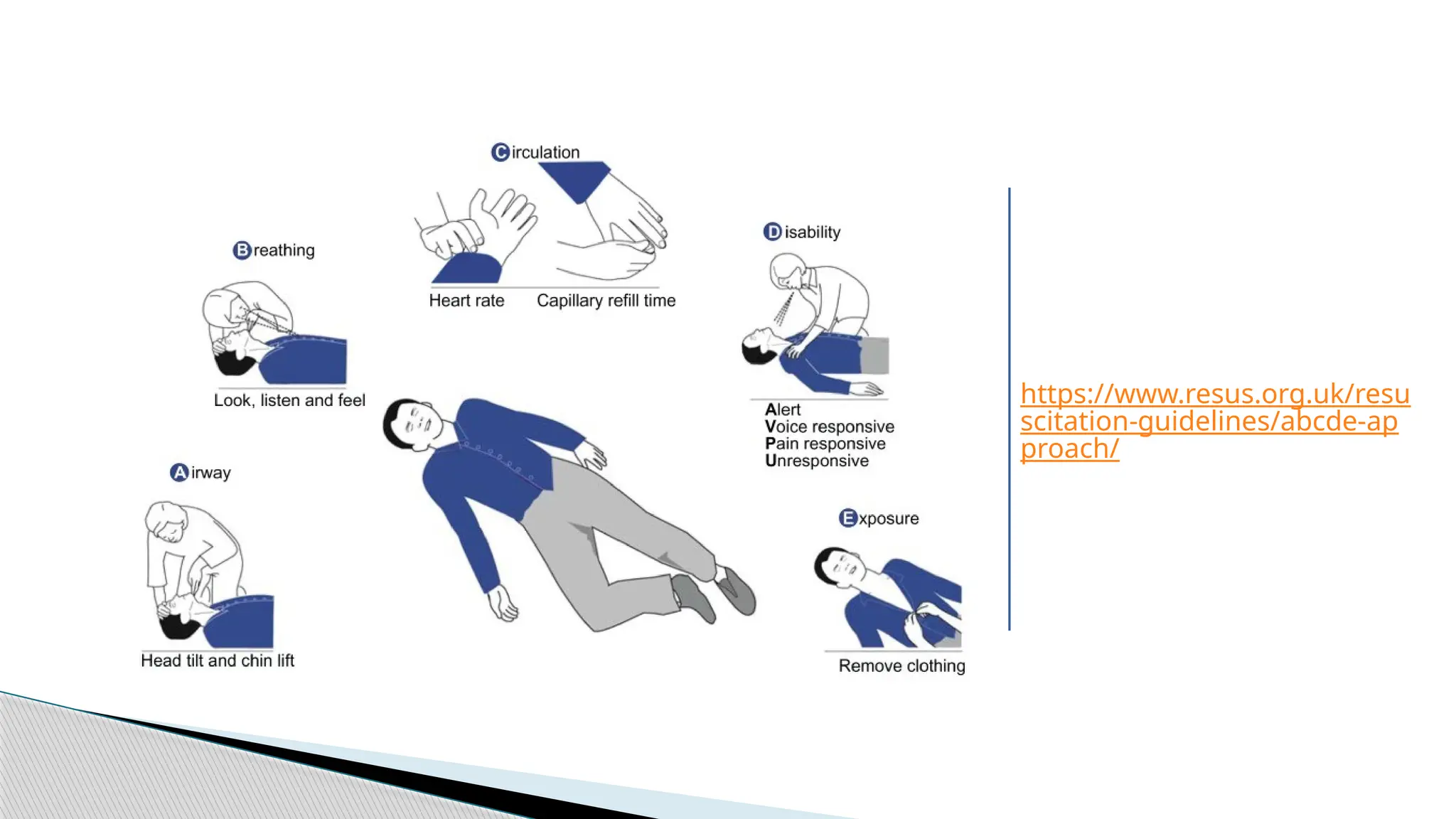
ABCDE Protocols
◦ Airway
◦ Breathing
◦ Circulation
◦ Disability
◦ Exposure
BLUE protocol: Bed Side Lung Ultrasonography in
Emergency.
FALLS Protocol: Fluid Administration Limited by Lungs
Sonography.
GCS scaling(15)
Assessment
Protocols
Main types
◦Obstructive Shock
◦ Cardiogenic Shock
◦ Distributive Shock
◦ Hypovolemic Shock
Types of Shock
10.
Actual physicalcause
Underlying pathology
Optimization of
◦ Cardiac output
◦ Blood pressure
◦ Oxygen delivery
Vascular tone restoration
Prevent any end organ failure
Or at least give supportive therapy
(pharmacological/prophylactic).
Generalized
Treatment
11.
Obstruction ofblood flow
into / out of the heart.
Impaired diastolic filling and
decreased cardiac output.
Causes:
◦ Pulmonary
◦ Circulatory occlusion
◦ Heart itself
Acute pericardial
tamponade,
Pulmonary or systemic
hypertension
Massive pulmonary emboli
occluding >50% of vascular
bed.
Obstructiv
e Shock
12.
CO isdecreased
CVP is elevated,
SVR is increased, and
Echocardiography is the definitive
diagnostic tool for Obstructive shock.
Diagnostic
Variables
13.
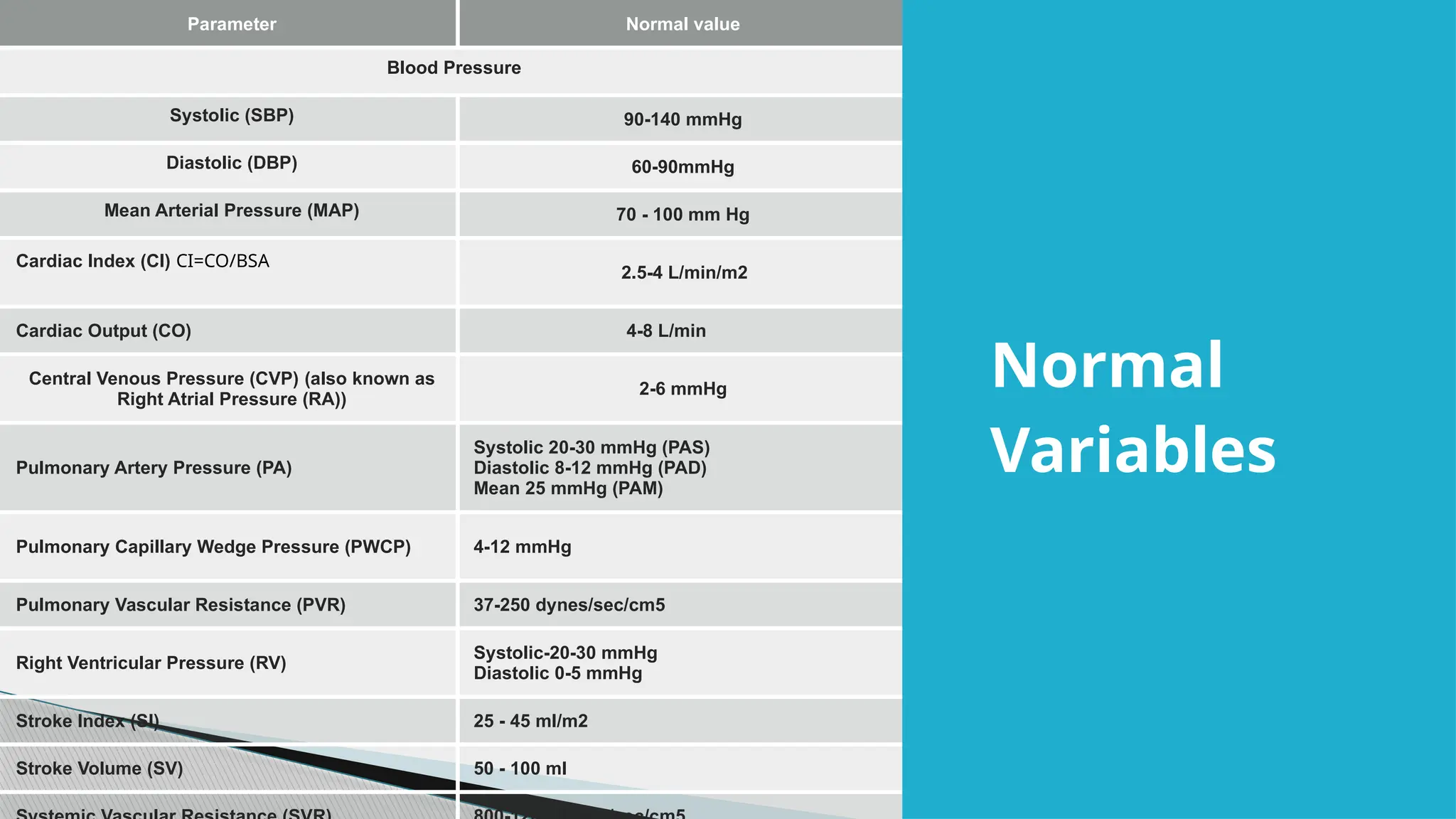
Parameter Normal value
BloodPressure
Systolic (SBP) 90-140 mmHg
Diastolic (DBP) 60-90mmHg
Mean Arterial Pressure (MAP) 70 - 100 mm Hg
Cardiac Index (CI) CI=CO/BSA
2.5-4 L/min/m2
Cardiac Output (CO) 4-8 L/min
Central Venous Pressure (CVP) (also known as
Right Atrial Pressure (RA))
2-6 mmHg
Pulmonary Artery Pressure (PA)
Systolic 20-30 mmHg (PAS)
Diastolic 8-12 mmHg (PAD)
Mean 25 mmHg (PAM)
Pulmonary Capillary Wedge Pressure (PWCP) 4-12 mmHg
Pulmonary Vascular Resistance (PVR) 37-250 dynes/sec/cm5
Right Ventricular Pressure (RV)
Systolic-20-30 mmHg
Diastolic 0-5 mmHg
Stroke Index (SI) 25 - 45 ml/m2
Stroke Volume (SV) 50 - 100 ml
Normal
Variables
14.
The symptomsof obstructive shock are considered emergencies because
they can lead to organ failure, tissue death, and death.
Symptoms that are associated with neurological function include confusion,
loss of consciousness, and inability to concentrate.
The symptoms that are related to the heart and its function are chest pain,
lightheadedness, and a sudden increase in heart rate along with a faint pulse.
Respiratory symptoms consist of shortness of breath and fast but shallow
breathing.
Other symptoms include sweating, decreased urine output, clammy skin,
pallor, and cold hands and feet.
Symptoms of Obstructive Shock
15.
As withall forms of shock, the management of obstructive shock should center around
the fundamental components for the treatment of shock.
The following should be considered:
◦ Positioning,
◦ Airway and breathing,
◦ Vascular access,
◦ Fluid resuscitation,
◦ Monitoring,
◦ Frequent reassessment,
◦ Lab studies,
◦ Medication therapy,
◦ Expert consultation.
Fundamentals of Shock Management:
16.
Occurs asa direct result of
myocardial dysfunction.
Heart failure to pump
adequately
Very rare to occur but often fatal.
Diminished Cardiac Output,
End organ hypoperfusion
Hypoxia
Cardiogenic
Shock
17.
Low myocardialcontractility
MI
Hypotension
Systemic vasodilation
Coronary artery disease
The hallmark is peripheral
vasoconstriction and vital end‐organ
damage, which stems from ineffective
stroke volume and insufficient
circulatory compensation.
This may, for a while, improve cardia
tissue perfusion but it increases the
afterload and workload on cardiac
muscle increases the damage.
Pathophysiol
ogy
18.
In thesetting of CS, classic ACS symptoms and
signs are combined with
◦ altered mental status,
◦ hypotension,
◦ arrhythmia,
◦ diminished pulses,
◦ dyspnea,
◦ peripheral edema,
◦ These features reflect an infarction involving
>40% of the left ventricle
Clinical Presentations
19.
The fourcommon clinical signs that
distinguish cardiogenic shock are
◦ Tachycardia,
◦ Dyspnea,
◦ Jugular vein distention,
◦ Hepatomegaly
Increased respiratory effort is often
the distinguishing characteristic
that sets cardiogenic shock apart
from other forms of shock.
Primary assessment model (ABCDE)
Airway:
◦ typically no airway abnormalities
and patent airway
Breathing:
◦ tachypena, and pulmonary
edema
Circulation:
◦ tachycardia, weak or
absent peripheral pulses,
jugular venous
distention, low BP with a
narrow pulse pressure,
delayed capillary refill,
signs of congestive heart
failure, and oliguria
Disability:
◦ anxiety, confusion,
restlessness, drowsiness,
and coma
Exposure:
◦ pale, cool, and
diaphoresis
Signs of
Cardiogenic
Shock:
Unlike other formsof shock which improve
with aggressive fluid resuscitation, rapid fluid
resuscitation with cardiogenic shock can be
counterproductive and may worsen the
patient’s condition.
Fluid overload and pulmonary edema may
occur.
Caution should be used when administering
fluids in the presence of cardiogenic shock.
Manageme
nt Of
Cardiogeni
c Shock
22.
Improve cardiac function.
Improvecardiac output.
Improve tissue perfusion.
Decrease myocardial oxygen demand.
Any drug that causes an
increase in systemic vascular
resistance (SVR) (afterload)
should be avoided.
This includes phenylephrine and
norepinephrine which both cause
potent vasoconstriction
Goals of
Manageme
nt
23.
Improve CardiacFunction
◦ Reduce SVR
◦ Dobutamine, milrinone, dopamine, and epinephrine
◦ Nitroprusside, which is a pure vasodilator, it may be necessary to use dopamine or
epinephrine to improve perfusion pressure when nitroprusside is administered.
◦ Diuretics may also be used if there is evidence of pulmonary edema or systemic venous
congestion.
Decreasing Oxygen Demand
◦ intubation and mechanical ventilation,
◦ maintenance of a normal temperature,
◦ and patient sedation.
Identification of the etiology is of primary importance because the etiology will
direct the course of treatment. Early expert consultation should be obtained.
Management Of Cardiogenic Shock
24.
Inotropic agents.You might be given medications to improve your heart function, such as
norepinephrine (Levophed) or dopamine, until other treatments start to work.
Aspirin. Emergency medical workers might give you aspirin immediately to reduce blood clotting
and keep your blood flowing through a narrowed artery. Take an aspirin yourself while waiting for
help to arrive only if your doctor has previously told you to do so for symptoms of a heart attack.
Thrombolytics. These drugs, also called clot busters or fibrinolytics, help dissolve a blood clot that's
blocking blood flow to your heart. The sooner you receive a thrombolytic drug after a heart attack,
the greater your chances of survival. You'll likely receive thrombolytics, such as alteplase (Activase) or
reteplase (Retavase), only if emergency cardiac catheterization isn't available.
Antiplatelet medication. Emergency room doctors might give you drugs similar to aspirin to help
prevent new clots from forming. These include medications, such as oral clopidogrel (Plavix), and
platelet glycoprotein IIb/IIIa receptor blockers, such as abciximab (Reopro), tirofiban (Aggrastat) and
eptifibatide (Integrilin), which are given through a vein (intravenously).
Other blood-thinning medications. You'll likely be given other medications, such as heparin, to
make your blood less likely to form clots. IV or injectable heparin usually is given during the first few
days after a heart attack.
Treatment of Cardiogenic Shock
25.
Angioplasty andstenting. If a blockage is found during a cardiac
catheterization, your doctor can insert a long, thin tube (catheter)
equipped with a special balloon through an artery, usually in your leg,
to a blocked artery in your heart. Once in position, the balloon is
briefly inflated to open the blockage.
A metal mesh stent might be inserted into the artery to keep it open
over time. In most cases, you doctor will place a stent coated with a
slow-releasing medication to help keep your artery open.
Balloon pump. Your doctor inserts a balloon pump in the main artery
of your heart (aorta). The pump inflates and deflates within the aorta,
helping blood flow and taking some of the workload off your heart.
Medical Procedures
26.
Coronary arterybypass surgery. This involves sewing veins or arteries in place
at a site beyond a blocked coronary artery. Your doctor might suggest this
procedure after your heart has had time to recover from your heart attack.
Occasionally, bypass surgery is performed on an emergency basis.
Surgery to repair an injury to your heart. Sometimes an injury, such as a tear
in one of your heart's chambers or a damaged heart valve, can cause
cardiogenic shock. Surgery might correct the problem.
Ventricular assist device. A mechanical device can be implanted into the
abdomen and attached to the heart to help it pump. This might extend and
improve the lives of some people with end-stage heart failure who are waiting
for new hearts or aren't able to have heart transplantation.
Heart transplant. If your heart is so damaged that no other treatments work, a
heart transplant may be a last resort
Surgical Procedure
27.
reduction inintravascular fluid volume.
◦ causes a decrease in stroke volume because of the resulting decrease in
preload
◦ Decreases cardiac output.
Causes
◦ Dehydration from vomiting and diarrhea,
◦ Hemorrhage,
◦ Decreased intake of fluids,
◦ Pathologic urinary losses (e.g. diabetic ketoacidosis, diabetes insipidus),
◦ Translocation of body fluids (e.g. burns, peritonitis, small bowel
obstruction).
Hypovolemic Shock
28.
Increased HR,
Increased afterload,
and/or Increased contractility.
Those are altered in compensation to hypovolemia, a viable
effort to maintain CO.
But alteration is the key to diagnose hypovolemic shock.
Compensatory Mechanisms In Hypovolemia
29.
The PrimaryAssessment acronym stands for Airway, Breathing, Circulation,
Disability, and Exposure.
A: Typically the airway of the child with hypovolemic shock will not be significantly
affected.
B: The patient may experience some Breathing changes and this may be
recognized by a nonlabored tachypnea. (With no effort)
C: The most notable changes will likely be seen with circulation. These circulation
changes include tachycardia, narrowing pulse pressure, possible systolic
hypotension, capillary refill time > 2 seconds, cool/pale skin, weak to absent
peripheral pulses, reduced urine output.
D: Disability or neurological changes include decreased level of consciousness.
E: Exposing the patient to observe the skin and extremities will often reveal cool,
pale, and mottled extremities
Sign and Symptoms (ABCDE Acronyms)
31.
• compensatory mechanismscan maintain systolic
blood pressure. This window of time is classified
as compensated shock.
If compensatory mechanisms fail and hypotensive
shock (low systolic BP) develops, the chances of
survival and recovery are significantly decreased
32.
◦ For 0- 10 kg = weight (kg) x 100 mL/kg/day.
◦ For 10-20 kg = 1000 mL + [weight (kg) x 50 ml/kg/day]
◦ For > 20 kg = 1500 mL + [weight (kg) x 20 ml/kg/day]
[Na+] in serum = TBS ÷ TBW ……………………………….equation 1
That means
TBS = [Na+] in serum x TBW ……………………………… equation 2
[Na+]high TBW1 = [Na+]desired (TBW1 + X)
∗ ∗
Where X is the free water deficit. If the desired sodium is 140, rearranging the equation and
solving for X gives you:
X = {([Na+]high – 140) ÷ 140 } TBW1
∗
TBW = Wt (kg) x 0.6 for males
TBW = Wt (kg) x 0.5 for females.
If elderly, use 0.5 for males and 0.45 for females.
To maintain their serum sodium concentrations at 140 mEq/L (140 mmol/L), infants also must
retain approximately 360 mEq (360 mmol) of sodium or 2 mEq/d (2 mmol/d).
Calculating fluid for Maintenance
33.
Excessive vasodilationand impaired distribution of blood flow.
Anaphylactic and septic shock
Neurogenic shock
Distributive Shock
34.
Hyperdynamic statedevelopment.
Inadequate tissue perfusion
Intraorgan shunting
Hypotensive state with increase mixed venous oxygen saturation.
Early Septic Shock (warm or hyperdynamic)
◦ Reduced diastolic Blood Pressure
◦ Flushed warm extremities
◦ Brisk capillary refill from peripheral vasodilation and increased cardiac output.
Late Septic Shock (cold or Hypodynamic)
◦ Decreased myocardial Contractility
◦ Paralyzed microvascular tone
◦ Pressure dependent reduction in organ perfusion (Hypoperfusion)
Pathophysiology
35.
Anaphylactic
◦ DecreasedSVR; histamine release from mast cells after activation of
antigen bound immunoglobulin (IgE)
◦ Increased prostaglandins
Neurogenic Shock
◦ Loss of sympathetic tone due to severe injury to the nervous system.
Pathophysiology (anaphylactic/ neurogenic)
36.
Anaphylaxis
◦ Respiratorydistress
◦ Wheezing
◦ Urticarial rashes
◦ Angioedema
◦ High grade fever in septic shock
Clinical Signs
37.
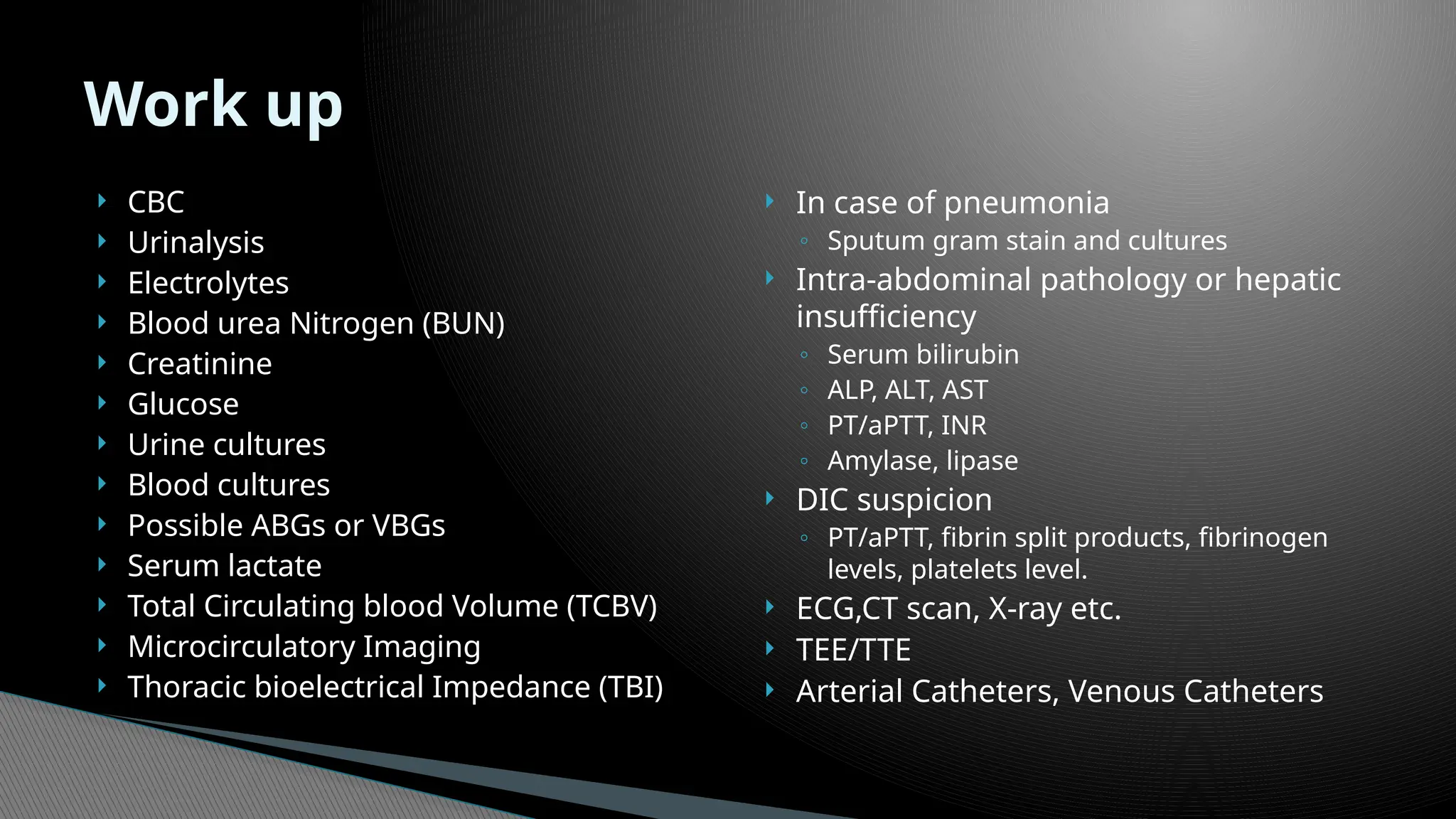
CBC
Urinalysis
Electrolytes
Blood urea Nitrogen (BUN)
Creatinine
Glucose
Urine cultures
Blood cultures
Possible ABGs or VBGs
Serum lactate
Total Circulating blood Volume (TCBV)
Microcirculatory Imaging
Thoracic bioelectrical Impedance (TBI)
In case of pneumonia
◦ Sputum gram stain and cultures
Intra-abdominal pathology or hepatic
insufficiency
◦ Serum bilirubin
◦ ALP, ALT, AST
◦ PT/aPTT, INR
◦ Amylase, lipase
DIC suspicion
◦ PT/aPTT, fibrin split products, fibrinogen
levels, platelets level.
ECG,CT scan, X-ray etc.
TEE/TTE
Arterial Catheters, Venous Catheters
Work up
38.
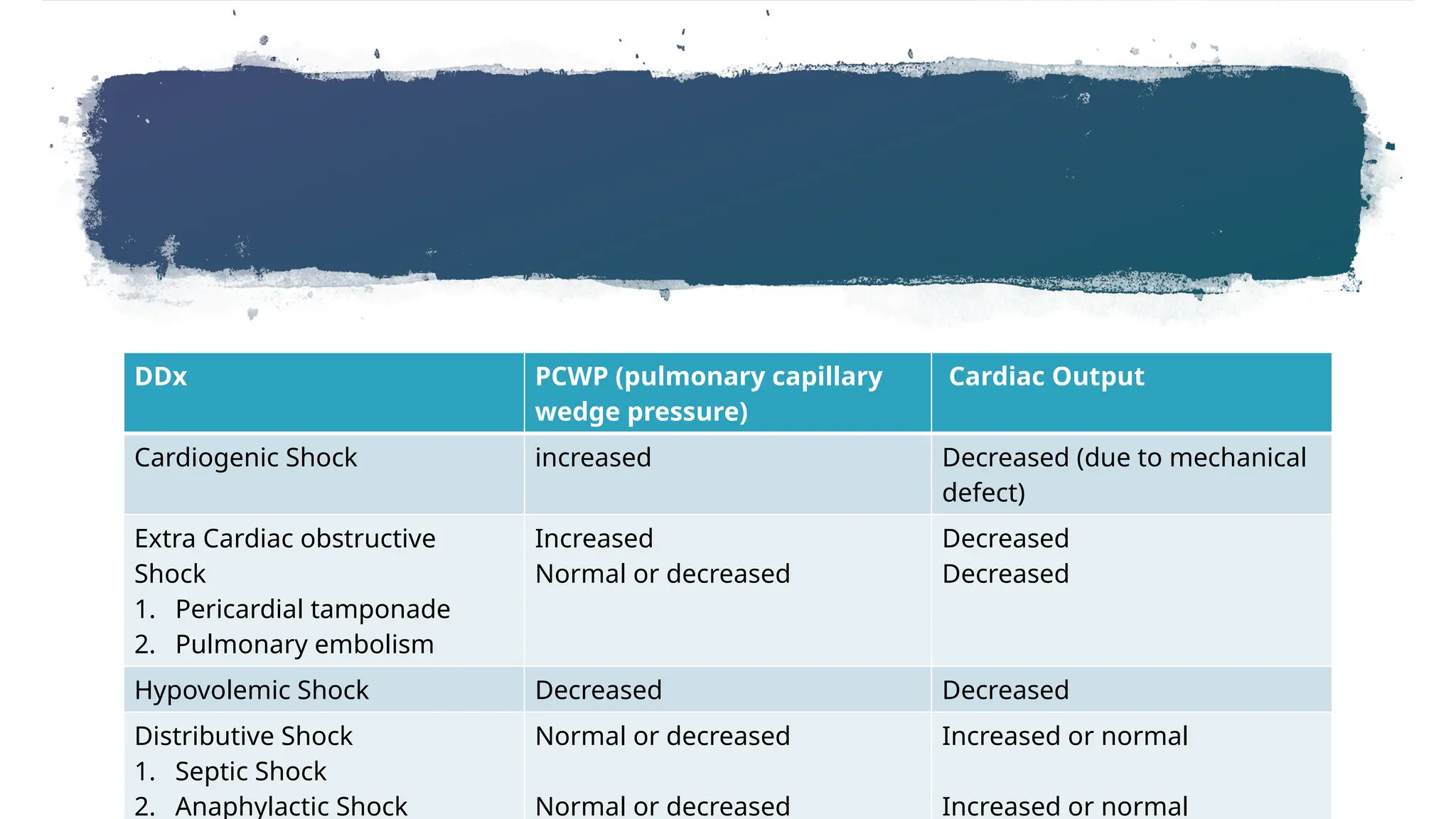
DDx PCWP (pulmonarycapillary
wedge pressure)
Cardiac Output
Cardiogenic Shock increased Decreased (due to mechanical
defect)
Extra Cardiac obstructive
Shock
1. Pericardial tamponade
2. Pulmonary embolism
Increased
Normal or decreased
Decreased
Decreased
Hypovolemic Shock Decreased Decreased
Distributive Shock
1. Septic Shock
2. Anaphylactic Shock
Normal or decreased
Normal or decreased
Increased or normal
Increased or normal
Editor's Notes
#3 Septic shock - This is caused by an overwhelming infection leading to vasodilation, such as by Gram negative bacteria i.e. Escherichia coli, Proteus species, Klebsiella pneumoniae which release an endotoxin which produces adverse biochemical, immunological and occasionally neurological effects which are harmful to the body. Gram-positive cocci, such as pneumococci and streptococci, and certain fungi as well as Gram-positive bacterial toxins produce a similar syndrome.
Anaphylactic shock - Caused by a severe anaphylactic reaction to an allergen, antigen, drug or foreign protein causing the release of histamine which causes widespread vasodilation, leading to hypotension and increased capillary permeability.
Neurogenic shock - Neurogenic shock is the rarest form of shock. It is caused by trauma to the spinal cord resulting in the sudden loss of autonomic and motor reflexes below the injury level. Without stimulation by sympathetic nervous system the vessel walls relax uncontrolled, resulting in a sudden decrease in peripheral vascular resistance, leading to vasodilation and hypotension.
![◦ For 0 - 10 kg = weight (kg) x 100 mL/kg/day.
◦ For 10-20 kg = 1000 mL + [weight (kg) x 50 ml/kg/day]
◦ For > 20 kg = 1500 mL + [weight (kg) x 20 ml/kg/day]
[Na+] in serum = TBS ÷ TBW ……………………………….equation 1
That means
TBS = [Na+] in serum x TBW ……………………………… equation 2
[Na+]high TBW1 = [Na+]desired (TBW1 + X)
∗ ∗
Where X is the free water deficit. If the desired sodium is 140, rearranging the equation and
solving for X gives you:
X = {([Na+]high – 140) ÷ 140 } TBW1
∗
TBW = Wt (kg) x 0.6 for males
TBW = Wt (kg) x 0.5 for females.
If elderly, use 0.5 for males and 0.45 for females.
To maintain their serum sodium concentrations at 140 mEq/L (140 mmol/L), infants also must
retain approximately 360 mEq (360 mmol) of sodium or 2 mEq/d (2 mmol/d).
Calculating fluid for Maintenance](https://image.slidesharecdn.com/lecture1shockanditsmanagement-250413132201-951daedf/75/Lecture-different-types-of-Shock-and-Its-Management-pptx-32-2048.jpg)