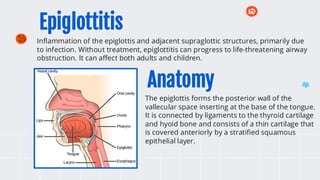
Epiglottitis
Inflammation of theepiglottis and adjacent supraglottic structures, primarily due
to infection. Without treatment, epiglottitis can progress to life-threatening airway
obstruction. It can affect both adults and children.
The epiglottis forms the posterior wall of the
vallecular space inserting at the base of the tongue.
It is connected by ligaments to the thyroid cartilage
and hyoid bone and consists of a thin cartilage that
is covered anteriorly by a stratified squamous
epithelial layer.
Anatomy
3.
Pathophysiology
Epiglottitis is mostfrequently caused by infection, although caustic ingestion, thermal
injury, and local trauma are important noninfectious etiologies.
Infectious epiglottitis is a cellulitis of the epiglottis, aryepiglottic folds, and other
adjacent tissues. It results from bacteremia and/or direct invasion of the epithelial
layer by the pathogenic organism through droplets of saliva or mucus.
The lingual surface of the epiglottis and periepiglottic tissues have networks of lymphatic
and blood vessels that facilitate the spread of infection. Once infection begins,
swelling rapidly progresses to involve the entire supraglottic larynx.
Two distinct mechanisms contribute to the development of stridor:
1- Supraglottic swelling reduces the caliber of the upper airway, causing turbulent airflow
during inspiration (stridor).
2- Posterior and inferior curling of the epiglottis due to airway obstruction.
4.
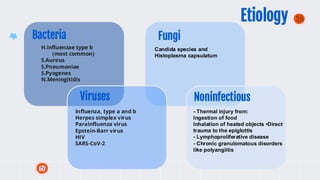
H.influenzae type b
(mostcommon)
S.Aureus
S.Pneumoniae
S.Pyogenes
N.Meningitidis
Bacteria
Viruses
Fungi
Noninfectious
Influenza, type a and b
Herpes simplex virus
Parainfluenza virus
Epstein-Barr virus
HIV
SARS-CoV-2
Candida species and
Histoplasma capsulatum
- Thermal injury from:
Ingestion of food
Inhalation of heated objects •Direct
trauma to the epiglottis
- Lymphoproliferative disease
- Chronic granulomatous disorders
like polyangiitis
Etiology
5.
Prevelance and Risk
•Incidence 0.63/100 000
• Anyone can develop epiglottitis.
• Several factors can increase the risk of
developing it:
- Age: age below 12 months children are at
high risk but the peak is between 2-6
years.
- Sex: male are more likely to get , but the
reason is not clear environment
- Heavily populated environments.
- Poor immune function makes it easier
for epiglottitis to develop.
- Having diabetes has been shown to be a
risk factor in adults
• Airway obstruction
• Cervical adenitis
• Empyema
• Epiglottic abscess
• Meningitis
• Pneumonia
• Pneumothorax
• Sepsis
• Septic arthritis
• Septic shock
• Vocal cord granuloma
• Ludwig angina-type submental infection
Complications
6.
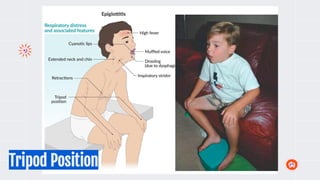
Clinical Manifestations
Young Children<5 years Older children,
adolescents, and adults
● respiratory distress, anxiety,
and the characteristic "tripod"
or "sniffing" posture. They
may be reluctant to lie down.
● Drooling is often present.
● Cough is typically absent.
● Severe sore throat.
● Dysphagia.
● Drooling.
● Relatively normal
● oropharyngeal examination;
and minimal respiratory
distress.
- Toxic appearance and distress (agitation,
restlessness, irritability)
- Sudden onset of high fever (between 38.8 and 40.0°C)
- Stridor
- Drooling
- Change in voice (muffled, "hot potato" voice)
Both
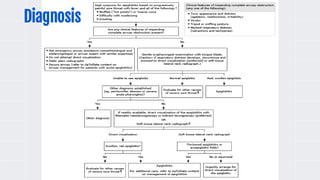
Diagnosis
• Clinical Symptoms.
•Directi visualization by Laryngoscopy.
• Soft-tissue lateral neck Radiographs.
• Laboratory studies should not be performed in young children with imminent
complete airway obstruction until the airway is secured because agitation caused
by pain may worsen respiratory distress and precipitate sudden respiratory arrest.
• Microbiology, Swabbing the epiglottis is difficult, potentially dangerous, and
contraindicated in patients who are not intubated.
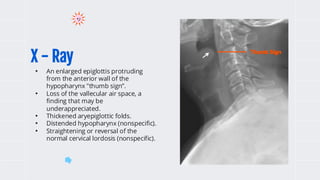
X - Ray
•An enlarged epiglottis protruding
from the anterior wall of the
hypopharynx "thumb sign”.
• Loss of the vallecular air space, a
finding that may be
underappreciated.
• Thickened aryepiglottic folds.
• Distended hypopharynx (nonspecific).
• Straightening or reversal of the
normal cervical lordosis (nonspecific).
Thumb Sign
11.
The annual incidenceof epiglottitis
among children has declined
dramatically since the introduction
of Hib vaccines (2-3 doses and a
booster dose), with the estimated
annual incidence of Hib as low as
two cases per 10 million children in
populations with high rates of
immunization. In addition, as Hib
has become a less frequent cause
of epiglottitis in children, it has
become more common among
school-age children and
adolescents than preschool
children (<5 years of age) .
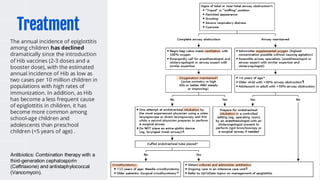
Treatment
Antibiotics: Combination therapy with a
third-generation cephalosporin
(Ceftriaxone) and antistaphylococcal
(Vancomycin).
12.
● Woods, C.R. (2023, December 20). Epiglottitis (supraglottitis):
Management. In R. M. Walls, G. C. Isaacson, & M. I. Neuman
(Section Eds.), J. F. Wiley II (Dep. Ed.). UpToDate.
https://www.uptodate.com
● Woods, C. R. (2023, December 20). Epiglottitis (supraglottitis):
Clinical features and diagnosis. In G. C. Isaacson & M. I. Neuman
(Section Eds.), J. F. Wiley II (Dep. Ed.). UpToDate.
https://www.uptodate.com
● Hindy, J., Novoa, R., Slovik, Y., Puterman, M., & Joshua, B. Z.
(2013). Epiglottic abscess as a complication of acute epiglottitis.
American Journal of Otolaryngology, 34(4), 362-365.
References