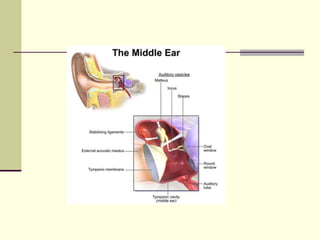
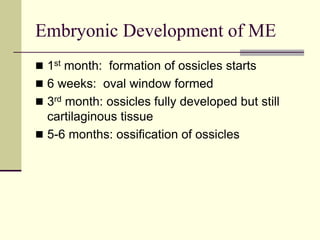
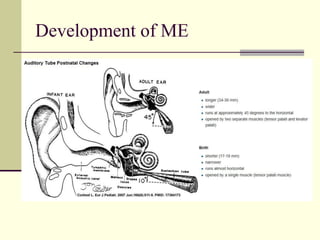
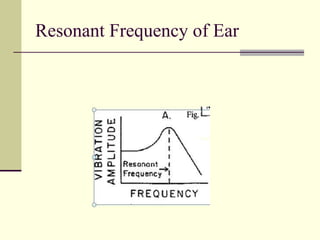
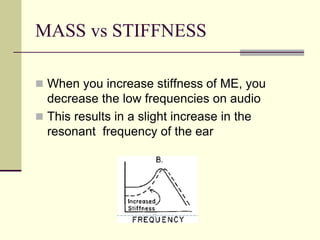
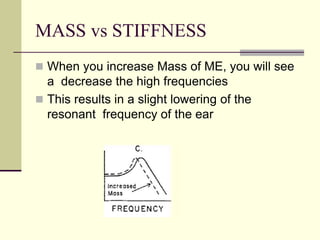
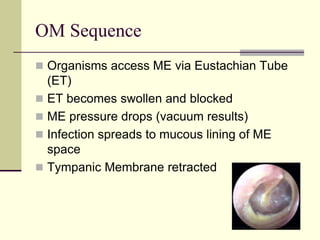
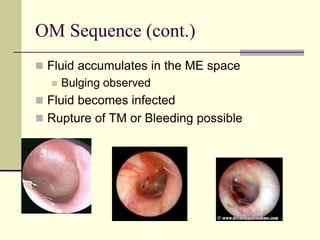
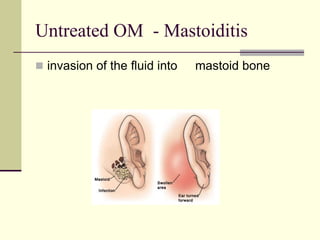
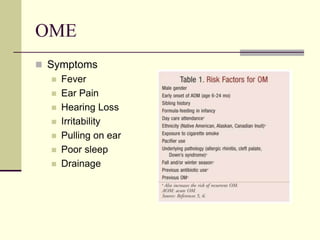
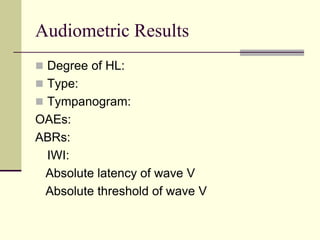
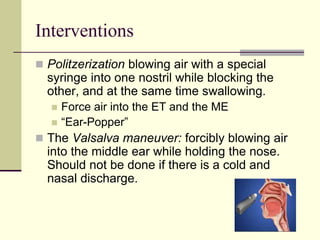
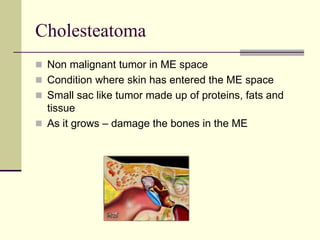
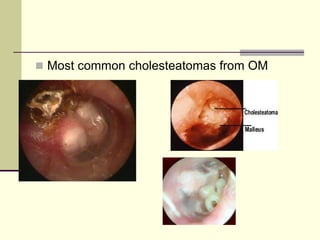
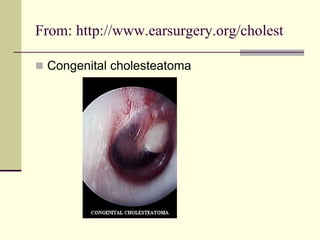
This document discusses several middle ear disorders including otitis media, mastoiditis, cholesteatoma, Bell's palsy, and otosclerosis. It describes the anatomy and development of the middle ear, how changes in mass and stiffness affect resonance, and symptoms, interventions, and audiometric results for each disorder. Common interventions discussed include antibiotics, PE tubes, myringotomy, politzerization, and surgery.