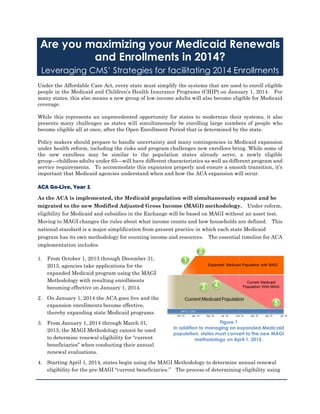
1. Figure 1
In addition to managing an expanded Medicaid
population, states must convert to the new MAGI
methodology on April 1, 2015.
Are you maximizing your Medicaid Renewals
and Enrollments in 2014?
Leveraging CMS’ Strategies for facilitating 2014 Enrollments
Under the Affordable Care Act, every state must simplify the systems that are used to enroll eligible
people in the Medicaid and Children’s Health Insurance Programs (CHIP) on January 1, 2014. For
many states, this also means a new group of low-income adults will also become eligible for Medicaid
coverage.
While this represents an unprecedented opportunity for states to modernize their systems, it also
presents many challenges as states will simultaneously be enrolling large numbers of people who
become eligible all at once, after the Open Enrollment Period that is determined by the state.
Policy makers should prepare to handle uncertainty and many contingencies in Medicaid expansion
under health reform, including the risks and program challenges new enrollees bring. While some of
the new enrollees may be similar to the population states already serve, a newly eligible
group—childless adults under 65—will have different characteristics as well as different program and
service requirements. To accommodate this expansion properly and ensure a smooth transition, it’s
important that Medicaid agencies understand when and how the ACA expansion will occur.
ACA Go-Live, Year 1
As the ACA is implemented, the Medicaid population will simultaneously expand and be
migrated to the new Modified Adjusted Gross Income (MAGI) methodology. Under reform,
eligibility for Medicaid and subsidies in the Exchange will be based on MAGI without an asset test.
Moving to MAGI changes the rules about what income counts and how households are defined. This
national standard is a major simplification from present practice in which each state Medicaid
program has its own methodology for counting income and resources. The essential timeline for ACA
implementation includes:
1. From October 1, 2013 through December 31,
2013, agencies take applications for the
expanded Medicaid program using the MAGI
Methodology with resulting enrollments
becoming effective on January 1, 2014.
2. On January 1, 2014 the ACA goes live and the
expansion enrollments become effective,
thereby expanding state Medicaid programs.
3. From January 1, 2014 through March 31,
2013, the MAGI Methodology cannot be used
to determine renewal eligibility for “current
beneficiaries” when conducting their annual
renewal evaluations.
4. Starting April 1, 2014, states begin using the MAGI Methodology to determine annual renewal
eligibility for the pre-MAGI “current beneficiaries.” The process of determining eligibility using
2. Figure 2
Following the ACA implementation state Medicaid agencies are faced with an enormous annual renewal
burden on January 1 when the newly enrolled expansion population renewals become due. Initial estimates
suggest this might amount to as much as 30% of the entire Medicaid population.
MAGI on “current beneficiaries” is completed by March 31, 2015.
5. Steady State will not be reached until Fiscal Year 2016.
Out-Year Annual Renewal Challenge
States face an increase in their annual Medicaid renewals one year after the ACA is
implemented. Because new ACA expansion enrollments commence on January 1, 2014, a spike in
annual renewals will occur on January 1 each year, starting in 2015. In January, 2015, the states
must complete annual renewals for Medicaid individuals who were added in January, 2014, adding
substantially to states’ workloads. Additionally, because current beneficiaries cannot be renewed
using the MAGI methodology until April, the January spike may be followed by a two month lull
before resuming renewals at a rate that could double the normal monthly renewal load.
Specific Targeted Enrollment Strategies
In its 5/17/2013 State Health Official (SHO) Letter, CMS outlined five specific targeted
enrollment strategies that states can use to facilitate Medicaid and CHIP Enrollments and
Renewals in 2014.
These Enrollment Strategies provide important advantages both for uninsured individuals as well as
states. They target individuals likely to be eligible for Medicaid, and for whom eligibility information
is already in the state’s files. As a result, states can use these strategies to easily identify and enroll
eligible individuals without requiring them to complete a new application. These strategies can also
be used to facilitate future renewals. As CMS suggests, these strategies help to alleviate the
increased administrative demands on the state’s eligibility and enrollment systems that are expected
during the Open Enrollment Period (10/1/2013 – 1/1/2014) and the first quarter of 2014.
Following are the five strategies noted in the 5/17/2013 SHO Letter:
3. 1. Implementing the early adoption of Modified Adjusted Gross Income (MAGI)-based rules.
2. Extending the Medicaid renewal period so that renewals normally occurring during the first
quarter of 2014 (January 1, 2014 – March 31, 2014) occur later.
3. Enrolling individuals into Medicaid based on Supplemental Nutrition Assistance Program
(SNAP) eligibility.
4. Enrolling parents into Medicaid based on their children’s income eligibility.
5. Adopting 12-month continuous eligibility for parents and other adults.
States can employ these enrollment strategies in order to dramatically mitigate the
post-ACA implementation renewal spikes. These strategies, coupled with other options such as
aligning Medicaid renewals with other program enrollments (e.g. SNAP & TANF) and structuring
policies to fully enable “No-Touch” renewals can help to smooth out this increase in renewal activity
and lessen its impacts on their Medicaid organizations.
While states may be hard-pressed by the many items on their Medicaid expansion task list, one item
can’t be put off: planning for smooth program operations in year 1 and the out-years.
This series of white papers analyzes each of these enrollment strategies and outlines the associated
benefits as well as some of the operational impacts of each.
4. Figure 3 During the 2013 Open Enrollment Period, states must use
two sets of rules to process new applications and 2013 Renewals.
and New Applications
Strategy 1 –
Implementing the early adoption of the Modified Adjusted Gross
Income (MAGI)-based rules.
The new Modified Adjusted Gross Income (MAGI) methodology differs from the Medicaid eligibility
rules that are currently in effect. Under the Affordable Care Act, states cannot simply replace their
current eligibility rules with MAGI. They must gradually transition to the new methodology.
Beginning October 1, 2013, states must use two sets of Eligibility Rules
During the Open Enrollment Period (October 1, 2013 through December 31, 2013), states must be able
to process new Medicaid applications with either MAGI or the current Medicaid rules. However, as
shown in Figure 3, states can only use the current Medicaid rules for renewals of their existing
Medicaid population that occur during
this period.
As a result, the states’ eligibility
systems and operational processes
must use two different sets of rules for
new Medicaid applications and
renewals of the existing Medicaid
population that occur during the Open
Enrollment Period.
Avoid using two sets of rules by adopting MAGI early
Strategy 1 allows states to fully adopt the MAGI methodology early during the Open Enrollment
Period for both 2013 Renewals as well as new applications. This allows states from having to operate
with two different sets of rules and enables them to better coordinate the new open enrollment process
with their traditional renewal process.
This strategy also allows states to better serve their existing beneficiaries who are found to be
ineligible. With synchronized processes, instead of simply terminating an ineligible beneficiary’s
coverage, states can immediately use the MAGI methodology assess the person’s eligibility for 2014
Medicaid or one of the state’s Qualified Health Plans.
What CMS requires
According to CMS’ 5/17/2013 State Health Official (SHO) Letter, in order to implement Strategy 1, a
state must have a time-limited section 1115 waiver of section1902(a)(17) of the Social Security Act
(the Act). This will allow them to use the new MAGI methodology for determining Medicaid
eligibility for people seeking coverage that will take effect prior to January 1, 2014.
CMS advises states who are interested in employing this strategy to also discuss this with CMS
during their regular State Operations and Technical Assistance (SOTA) calls.
5. Figure 4 During the first quarter of 2014, states must use two sets
of rules to process 2013 Renewals.
Strategy 2 –
Extending the Medicaid renewal period.
The Affordable Care Act contains a provision that protects current Medicaid recipients from losing
their eligibility solely because of the new MAGI methodology and new household composition rules
that are implemented in 2014. This provision
focuses on renewals that occur during the first
quarter of 2014 (January 1, 2014 through March
31, 2014) and requires states’ renewal processes
to test eligibility with two sets of rules.
For first quarter of 2014 renewals, states must use two sets of Eligibility Rules
During the first quarter of 2014 (January 1, 2014 through March 31, 2014), states will only use the
MAGI methodology for all new Medicaid applications. However, as shown in Figure 4, for renewals
of their existing Medicaid populations that occur during this period, states must also be able to use the
current Medicaid rules. Because of the
protection provision, if a beneficiary is found
to be ineligible because of the MAGI
methodology, the state must conduct
another eligibility assessment with the
current pre-MAGI rules that are in place
today.
As a result, the states’ eligibility systems
and operational processes must be able to apply both current pre-MAGI rules and MAGI rules to all
beneficiaries whose renewal date falls between January 1 and March 31, 2014.
Avoid using two sets of rules by simply deferring 1st Quarter 2014 Redeterminations
Strategy 2 allows states to extend the Medicaid renewal period for beneficiaries whose coverage is up
for renewal in the first quarter of 2014. This enables state to delay renewal dates so that they occur
after March 31, 2014, the last date of the Affordable Care Act’s protection provision.
This frees the states from having to use two sets of eligibility rules for redeterminations that occur
from January 1, 2014 through March 31, 2014 and thereby limit of the risk of mistakes and
inefficiencies. As a result of this strategy, states would not have to conduct renewals in the first
quarter of 2014 and need only use the MAGI methodology rules for all renewals that are scheduled to
occur after March 31, 2014.
As part of Strategy 2, states would be able to define how the delays would occur. For example, using
a delay of 90 days for this period would result in renewals that are scheduled for January 2014 to
occur in April 2014, renewals slated for February 2014 would occur in May 2014, and renewals
scheduled for March 2014 would occur in June 2014. This flexibility allows states to evenly
distribute these rescheduled renewals in a way that matches the capacity of the organization.
What CMS requires
According to CMS’ 5/17/2013 State Health Official (SHO) Letter, Section 1902(e)(14)(A) of the
Affordable Care Act, added by section 2002 of the Affordable Care Act, generally requires the use of
the MAGI-based income methodology to determine Medicaid eligibility, and also allows for waivers “as
6. are necessary to ensure that states establish income and eligibility determination systems that protect
beneficiaries.” As a result, states that are interested in using Strategy 2 can request such waiver
authority under section 1902(e)(14)(A) of the Act on a time-limited basis. The Strategy 2 waivers are
not subject to transparency rules and, as a result, no additional procedures are required by federal
law.
CMS advises states who are interested in employing this strategy to also discuss this with CMS
during their regular State Operations and Technical Assistance (SOTA) calls.
7. Strategy 3 --
Enrolling individuals into Medicaid based on Supplemental Nutrition
Assistance Program (SNAP) eligibility.
In general, most people who are currently enrolled in SNAP would be eligible for Medicaid. This is
because, in order to qualify for SNAP, a household’s gross income cannot exceed 130 percent of the
federal poverty level
SNAP is a trusted and complementary program
In many states, income data from SNAP is considered to be
reliable because it is stringently verified and in most cases is no
more than 6 months old. As a result, SNAP income data is often
used to renew Medicaid eligibility.
Use SNAP data to quickly enroll SNAP participants who are eligible for Medicaid
Strategy 3 allows states to facilitate the Medicaid enrollment of non-elderly, non-disabled SNAP
participants who are financially eligible with the new MAGI methodology. States can benefit from
this strategy because it allows them to enroll eligible SNAP participants directly into Medicaid
without having to conduct additional determinations that are based on the new MAGI rules.
From a systems and operational perspective, Strategy 3 helps states who are implementing new
eligibility systems. Since it provides a trusted and direct path for enrolling people in Medicaid,
Strategy 3 helps states to relieve some of the pressure and increased volume that will be placed on
their new systems and processes beginning on October 1, 2013.
From an outreach and customer service perspective, this strategy also helps inform SNAP
participants of their Medicaid eligibility and provides them with a clear and easy way for them to
enroll. Since SNAP participants already have trusted relationships with their states, with this
strategy, they do not have to work with an approved Navigator who may be unknown to them or visit
their state’s marketplace to apply for Medicaid. This is because much of their trusted SNAP data
satisfies most of the information that is required by the new single, streamlined application for
Medicaid.
Operational Considerations
In order to enroll eligible SNAP participants, states must still obtain the minimum required amount
of information for a Medicaid application. In addition to the SNAP application data that is already
on file and can be easily transferred to the Medicaid program, this includes a signature that meets the
requirements of the Affordable Care Act.
In its 5/17/2013 SHO Letter, CMS outlined the following options that could be used to attain this
signature from eligible SNAP participants:
a. The household applies for Medicaid through the SNAP application by using a check-box that
has been added to the SNAP enrollment form.
b. The household applies for Medicaid at its SNAP recertification by using a check-box that has
been added to the SNAP recertification form.
8. c. Non-elderly, non-disabled household members receive a Medicaid card at the time the SNAP
household is notified of SNAP enrollment or recertification. A phone call or online
acknowledgement by an adult who receives a card constitutes a Medicaid application and
“activates” the card.
d. Non-elderly, non-disabled household members receive a Medicaid card at the time the SNAP
household is notified of SNAP enrollment or recertification. These household members
indicate that they are applying for Medicaid when they go through the process of selecting a
managed care plan. This process also activates the Medicaid card.
Some states have also developed a series of notices that informs SNAP participants of their eligibility
for Medicaid and asks if they would like to be enrolled in Medicaid. SNAP participants who sign the
notice, indicate that they would like to be enrolled, and return the notice to the state are then enrolled
into Medicaid. (As part of this normal Medicaid enrollment process, these participants also receive a
formal Notice of Eligibility as well as a Medicaid card.)
What CMS requires
According to CMS’ 5/17/2013 State Health Official (SHO) Letter, in order to implement Strategy 3, a
state must request a waiver under section 1902(e)(14)(A) authority to allow the state to enroll eligible
non-elderly, non-disabled SNAP participants who are not already enrolled in Medicaid.
The state will have to explain why such a procedure is necessary to help implement its eligibility and
enrollment system as well as meet its administrative responsibilities for the program. In addition to
this, the state will have to define the timeframe during which it will use this strategy and must
explain how it will obtain the minimum requirements for an application to be enrolled in Medicaid
under 42 CFR 435.907, including the requirement to obtain a signature, whether physical, electronic
or telephonic, that complies with the requirements under 42 CFR 435.907(f).
9. Strategy 4 --
Enrolling parents into Medicaid based on children’s income eligibility
All states cover some parents through Medicaid, but the eligibility threshold for parents is often very
low. When the Affordable Care Act (ACA) is fully implemented, Medicaid eligibility will be extended
to most adults, including parents, with incomes up to 138 percent of the FPL.
For states who are expanding their Medicaid programs by adding the new adult group under
1902(a)(10)(A)(i)(VIII) of the Affordable Care Act, a large number of parents whose children are
already enrolled in Medicaid are likely to meet the new MAGI-based income eligibility standards.
Many parents of children currently enrolled in Medicaid will be eligible for coverage in
states that expand their Medicaid program
With these facts in mind, CMS is offering states an opportunity to facilitate the Medicaid enrollment
of parents whose children are currently enrolled in Medicaid and who are likely to be
Medicaid-eligible. This will help states to provide an efficient way to enroll adults in Medicaid and
will relieve some of the operational pressures that will occur as states progress through the initial
phases of implementing new eligibility and enrollment systems.
Strategy 4 enables states to facilitate the enrollment of parents of children currently enrolled in
Medicaid. States would have to identify all families with incomes at some level below 138 percent of
the federal poverty level who are likely to be Medicaid-eligible. Using a standardized and approved
process for converting the states’ current Medicaid effective income standards to new MAGI-based
income standards will help the states to identify income levels for households that are likely to be
Medicaid-eligible.
Operational Considerations
In order to enroll eligible parents, states must still obtain the minimum required amount of
information for a Medicaid application. In addition to the child’s Medicaid application data that is
already on file and can be easily transferred to the Medicaid program, this includes a signature as well
as additional non-financial information that are necessary to make an eligibility determination.
CMS has specified that states could use a combination of actions similar to the ones described in
Strategy 3 to collect this additional non-financial information and obtain a signed application from the
parents of children who are already enrolled in Medicaid.
In its 5/17/2013 SHO Letter, CMS also outlined the following approaches for attaining signatures from
eligible parents:
a. States that are extending Medicaid eligibility to the new adult group can reactivate existing
applications for parents who recently applied for Medicaid and were denied. If a parent has
applied for Medicaid recently (for example, up to 90 days prior to the 2013 open enrollment
period), but has been denied because his or her income exceeded the Medicaid income limit
then in effect, the state may send a notice indicating the application has been reactivated. If
the parent’s income is below the level for which the state has declared it will use for Strategy 4,
the state could subsequently enroll the parent.
10. b. States can review children’s Medicaid cases to identify parents who have not applied for
themselves, but who are likely to be eligible based on having income below the level for which
the state has declared it will use for Strategy 4. The state can send such parents a notice
informing them that they now may be eligible for Medicaid and requesting any necessary
missing information. The state can then determine eligibility and enroll eligible parents.
What CMS requires
According to CMS’ 5/17/2013 State Health Official (SHO) Letter, in order to implement Strategy 4, a
state must request a waiver under section 1902(e)(14)(A) authority to allow the state to enroll parents
whose children are financially eligible for Medicaid at levels indicating likely parental eligibility, and
who meet other non-financial Medicaid requirements (such as citizenship documentation).
The state will also have to explain why such a procedure is necessary to help implement its eligibility
and enrollment system as well as meet its administrative responsibilities for the program. In
addition to this, the state will have to define the timeframe during which it will use this strategy.
11. Strategy 5 --
Adopting 12-month continuous eligibility for parents and other adults
Within current Medicaid regulations, states are allowed to provide 12 months of continuous eligibility
to children in their Medicaid and CHIP programs. This enables states to protect children by
guaranteeing that they are able to retain coverage for 12 months regardless of changes in family
circumstances such as household or income changes. It also allows states to provide children with a
secure source of health insurance and safeguards against interruptions to ongoing care. According to
CMS, as of January 2013, 32 states have adopted 12-month continuous eligibility in their Medicaid or
CHIP programs for children, with 23 states implementing the option in both programs
The 12-month continuous eligibility provision mitigates “churning”
Strategy 5 enables states to extend this continuous eligibility provision to parents and other adults.
As a result, this strategy allows states to protect adult Medicaid beneficiaries in the same way that
children are protected with this option. From a state’s operational perspective, this option also helps
to mitigate problems associated with the enrollment and re-enrollment of eligible people when they
lose coverage due to frequent changes in income. (This is also known as “churning.”)
Also, CMS notes that Strategy 5 allows states to better coordinate coverage for whole families,
especially in states that otherwise would have 12-month continuous eligibility only for children.
Otherwise, in these states, parents might have to renew their coverage more frequently than children.
What CMS requires
According to CMS’ 5/17/2013 State Health Official (SHO) Letter, in order to implement Strategy 5, a
state is required to acquire section 1115 demonstration authority. CMS requires states with existing
demonstrations to submit an amendment request along with a revised budget neutrality agreement
that includes the financial impact on the demonstration as a result of the amendment. States that do
not have existing section 1115 demonstrations would have to submit an application for a new
demonstration. New requests will need to conform to the section 1115 demonstration transparency
rules at 42 CFR 431.412(a).
12. As states work to meet their project goals and schedules associated with their initiatives to meet the
important tenants of the Affordable Care Act, CMS is serving as a willing partner to help states
improve their programs as well as deal with the pressures associating with implementing new
systems and processes. These strategies help states to provide additional pathways to enable eligible
individuals to gain access to Medicaid and achieve many of the key objectives of the ACA.
CAI is a global firm with a strong Public Sector practice focusing on assisting clients with their most
critical needs including Medicaid program changes and leveraging each of these 5 strategies.
CAI has been growing for over 27 years and today is comprised of more than 2,500 professionals. We
have offices throughout the United States, Canada, Europe, and the Asia-Pacific region, and industry
expertise in the Public Sector, Manufacturing, Insurance, Utilities, Hospitality, Logistics, Financial
Services, and Pharmaceuticals industries.
For more information about how CAI can help
you with your HHS needs please contact:
Joanne Gallagher
Director, Public Sector Practice
Joanne_Gallagher@compaid.com
Todd Schrubb
Director, Public Sector Practice
Todd_Schrubb@compaid.com