
Recommended
More Related Content
Similar to InstructionsPart 8 Stakeholder Engagement Monitor and Control P
Similar to InstructionsPart 8 Stakeholder Engagement Monitor and Control P (20)
More from TatianaMajor22
More from TatianaMajor22 (20)
Recently uploaded
Recently uploaded (20)
InstructionsPart 8 Stakeholder Engagement Monitor and Control P
- 1. Instructions Part 8: Stakeholder Engagement Monitor and Control Plan For the project selected in Unit I, create a simple stakeholder engagement monitor and control plan. Your plan should follow the process for managing and monitoring stakeholder engagement, as referred to in Figures 9.1 and 9.2 in the textbook. Your plan should include an introduction, and should answer the following questions: · What specific soft skills will you employ in managing project stakeholders? · What ground rules will you establish for managing project stakeholders? · What types of meetings do you plan to have with project stakeholders? How often do you plan to hold them? · How will you manage change requests from stakeholders? · How will you monitor stakeholders and levels of stakeholder engagement? · How will you manage changes to stakeholder requirements? · What historical documents will you update in the process of managing and monitoring stakeholders? Create the stakeholder management and control plan that addresses the questions above. Feel free to use tables, graphics, or document template examples to summarize your policy and approach. As a guide to depth, your stakeholder management and control plan should be a minimum of two pages in length. If you use tables, you may either create your table in Word and include it at the end of the document, or submit it as a separate Excel file. Adhere to APA Style when constructing this assignment, including in-text citations and references for all sources that are used. Please note that no abstract is needed.
- 2. Instructions Course Project, Executive Summary For the project selected in Unit I, prepare a PowerPoint presentation of a minimum of 10 slides to provide an executive summary briefing. The minimum number of slides does not count the title slide or the references slide. The presentation should summarize each part of the course project that you developed throughout this course. The goal of the briefing PowerPoint presentation is to offer a succinct yet comprehensive view of your project stakeholder and communication plan. This includes the following elements: · Part 1: Project Selection, Stakeholder Identification, And Stakeholder Analysis · Part 2: Resource Management Plan and RACI (responsible, accountable, consulted, and informed) Chart · Part 3: Communication Plan · Part 4: Stakeholder Plan · Part 5: Resource Acquisition Plan · Part 6: Team Development Plan · Part 7: Team Performance Reporting · Part 8: Stakeholder Engagement Monitor and Control Plan (from the assignment also in this unit) Adhere to APA Style when constructing this assignment, including in-text citations and references for all sources that are used.
- 3. Establishing an Integrated Care Practice in a Community Health Center Andrea Auxier and Tillman Farley Salud Family Health Centers, Fort Lupton, Colorado and University of Colorado, Denver Katrin Seifert Salud Family Health Centers, Fort Lupton, Colorado In a progressively complex and fragmented health care system and in response to the need to provide whole-person, quality care to greater numbers of patients than ever before, primary care practices throughout the United States have turned their attention and efforts to integrating behavioral health into their standard service-delivery models. With few resources and little guidance, systems struggle to gather the support required to establish effective integrated programs. Based on first-hand experience, we describe a working integrated primary care model, currently utilized in a large community health center system in Colorado, that encompasses
- 4. universal screening, consultation, psychotherapy, and psychological testing. With appreciation for the way an organization’s unique circumstances inform the best approach for that particular organization, we highlight the clinical- level and system-level variables that we consider necessary for successful practice development and address how our behavioral health program operates despite funding limitations. We conclude that organizations that aim for integrated primary care must mobilize leadership to implement systemic changes while making difficult decisions about program development, financing, staffing, and interagency relationships. Keywords: integrated care, primary care, integrative medici ne, health psychology, collaborative care The health care system in the United States is facing a paradox of declining outcomes and rapidly increasing costs (Rabin et al., 2009). In 2008, mental health conditions accounted for $72 billion in expenditures, making them the third most costly group of conditions (along with cancer), exceeded only by heart conditions and trauma-related disorders or conditions (Agency for Healthcare Research & Quality, 2008). In an effort to improve the provision of health care, many experts and key organizations are lending support to the movement for integration of behavioral health into primary care settings (Blount, 2003; Institute of Medicine, 2001, 2006; Pincus, 2003; U.S. Department of Health and Human Ser-
- 5. vices, 2006; World Health Organization & World Organization of Family Doctors, 2008). Numerous studies have demonstrated that integrated services can improve access to mental health care, enhance quality of care, decrease health care costs, improve over- all health, decrease the burden on primary care providers (PCPs), and improve PCPs’ ability to address patients’ mental health needs (Butler et al., 2008; Chiles, Lambert, & Hatch, 1999; O’Donohue, Cummings, & Ferguson, 2003; World Health Organization & World Organization of Family Doctors, 2008). The decision to organize integration efforts at our community health center was, in part, based on well-known data regarding primary care patients. For example, psychiatric conditions are common in patients who are seen in primary care practices (Cwikel, Zilber, Feinson, & Lerner, 2008) and many patients who have mental health needs seek treatment for these concerns through their PCP (Goldman, Rye, & Sirovatka, 2000; Petterson et al., 2008; Wang et al., 2006). Additionally, the majority of medical problems seen in primary care practices are undeniably linked with behaviors, and it has been estimated that 40% of premature deaths in the United States are attributable to health behavior factors (McGinnis & Foege, 1993; Mokdad, Marks, Stoup, & Gerberding, 2004). Behavioral health integration is an integral part of a solution
- 6. to the complex health care needs of these patients. Although the terms mental health and behavioral health are sometimes used interchangeably, we conceptualize them as differ- ent constructs. The term behavioral health applies to patients whose primary diagnosis is somatic and whose psychological symptoms, if present, are subclinical and related to the primary diagnosis. The term mental health applies when the focus of treatment is psychiatric; there may or may not be an accompanying This article was published Online First August 29, 2011. ANDREA AUXIER received her PhD in clinical psychology from the Uni- versity of Massachusetts, Boston. She is Director of Integrated Services and Clinical Training at Salud Family Health Centers and a senior clinical instructor at the University of Colorado, Denver, Department of Family Medicine. Her areas of professional interest include integrated primary care research and practice, especially as they apply to immigrant populations with trauma histories. TILLMAN FARLEY received his MD from the University of Colorado, School of Medicine, and completed his residency at the University of Rochester. He is board certified in Family Medicine. He is the Medical Services Director at Salud Family Health Centers and an associate professor at the University of Colorado, Denver, Department of Family Medicine. His
- 7. areas of professional interest include integrated primary care and health disparities, particularly as they apply to immigrant populations. KATRIN SEIFERT received her PsyD in clinical psychology from the Uni- versity of Denver. She is the Associate Psychology Training Director at Salud Family Health Centers. Her areas of professional interest include practice and clinical training in integrated primary care as well as complex trauma. CORRESPONDENCE CONCERNING THIS ARTICLE should be addressed to Katrin Seifert, Salud Family Health Centers, P.O. Box 189, Frederick, CO 80530. E-mail: [email protected] Professional Psychology: Research and Practice © 2011 American Psychological Association 2011, Vol. 42, No. 5, 391–397 0735-7028/11/$12.00 DOI: 10.1037/a0024982 391 T hi s do cu m en t i
- 10. le is in te nd ed s ol el y fo r t he p er so na l u se o f t he in di
- 12. medical condition. In this article, however, the term behavioral health will subsume both categories. Integrated Primary Care at Salud Family Health Centers Founded in 1970, Salud Family Health Centers (Salud) is a federally qualified community health center consisting of nine health care clinics covering eight counties in North Central Colo- rado. Salud is an important part of the health care safety net, providing population-based, fully integrated medical, dental, and behavioral health services regardless of finances, insurance cov - erage, or ability to pay–Salud focuses on the needs of the medi- cally indigent, uninsured, and underinsured populations. The na- tional distribution of payer sources for federally qualified health centers is 35% Medicaid and 25% Medicare or private insurance, with 40% of patients falling into the uninsured category (Adashi, Geiger, & Fine, 2010). By comparison, 30% of Salud’s patients have Medicaid, 14% have Medicare or private insurance, and 56% are uninsured, leaving Salud to support the health care of a greater proportion of patients with no funding source. Salud employs 540 individuals, including 60 medical providers, 14 dentists, 9 dental hygienists, and 15 behavioral health providers (BHPs). In 2010, Salud served more than 80,000 patients with
- 13. approximately 300,000 visits, making it the second largest health care provider in a six-state region. The most common visit types include well-child checks, prenatal visits, diabetes, and hyperten- sion. About 3,000 of Salud’s patients are migrant and seasonal farmworkers, and 65% of patients are Latino, many of whom speak Spanish as their primary or only language. In response to the extraordinary number of patients with behav- ioral health needs, immigration-related stressors, and limited fi- nancial means, Salud’s move toward integration began in 1997 under the leadership of its medical director, who had received training in an integrated model. The need for integration was apparent, but it soon became clear that incorporating a team of behavioral health providers into an established medical setting was a more complex proposition than it initially seemed. The program started with one BHP in one clinic. PCPs who found value in the service vocalized their desire for an expanded behavioral health presence. As Salud hired more BHPs, it became necessary to build an infrastructure designed to support integration at an organiza- tional level. We set out to create a service-delivery model and develop job descriptions, billing and coding practices, policies, protocols, standard operating procedures, and data tracking mech- anisms. In order to accomplish these tasks, the focus shifted toward securing administrative support from key members of the organization. Over time, with the collective mission to provide quality health care—and with the implicit acceptance that behav- ioral health needs must be addressed as part of its delivery—
- 14. efforts materialized into an integrated care program. In an effort to measure the effectiveness of our program, we recently have begun to work toward an information-technology-driven, outcome- based approach, whereby we collaborate with university partners to measure and benchmark our data through regional and national comparative effectiveness research networks. In 2010, we developed a mission statement that reads: “To deliver stratified, integrated, patient-centered, population-based services utilizing a diversified team of behavioral health profes - sionals who function as PCPs, not ancillary staff, and who work shoulder-to-shoulder with the rest of the medical team in the same place, at the same time, with the same patients.” The implications of this mission include that BHPs have the ability to see a patient at any time, for any reason, without requiring a consult request from a PCP. This approach requires a paradigm shift from a superior/subordinate mentality to one of implicit understanding of the unique skills that all persons involved in the patient’s care contribute to the patient’s overall well-being. It gives BHPs the latitude to determine which patients they need to assess on a given day, and providers see each patient as “our patient” not “my patient.” Components of Integrated Care Over time, we have become familiar with many factors that influence the development, success, and sustainability of an
- 15. inte- grated primary care practice. Below is a summary of what we have found to be essential components of integration, broken down into those variables related to clinical decisions and interventions and those related to system-level considerations. Clinical Variables One prospect of integration is the provision of real time inter - ventions. As soon as a need is identified, a BHP is present to provide services. PCPs who might otherwise shy away from un- covering mental health issues are less likely to do so if they know they can call upon a BHP to address identified concerns. Just as some primary care visits are considered urgent, so are some behavioral health visits. Having a BHP available when these situations arise can mean that a patient actually receives care as opposed to falling through the cracks in a health care system in which timely access is often a problem (Pincus, 2003; Strosahl, 1998). In any large primary care system, behavioral health services must be population-based and not disease specific. A population- based approach focuses on the needs of a defined community with an emphasis on evidence-based practice and effective outcomes as well as primary prevention (Ibrahim, Savitz, Carey, & Wagner, 2001). In order to meet the needs of an entire community, BHPs must be capable of assessing and addressing multiple presenting concerns of varying levels of severity. BHPs in primary care cannot be limited to utilizing interventions that target only a
- 16. specific disease category, primarily because comorbidity is the rule rather than the exception (Klinkman, 2009). In response to this reality, treatment approaches must be geared toward the whole person, not the illness. BHPs who work in a primary care setting need to have strong generalist training, with sufficient understanding of normal and abnormal developmental processes across the life span, and to be flexible. The nature of the setting requires BHPs to make instant connections with patients, to formulate quick assessments, and to communicate the relevant findings to the PCP immediately. From a logistical standpoint, BHPs must be willing to swap the comfort and controllability of a therapy room for the unpredictable and unsettling reality of seeing patients in the medical rooms, often with interruptions. 392 AUXIER, FARLEY, AND SEIFERT T hi s do cu m en t i s
- 19. is in te nd ed s ol el y fo r t he p er so na l u se o f t he in di vi
- 21. System Variables Colocation is crucial for successful integrated primary care (Blount, 2003). For integration to be truly seamless, the BHP must be in the flow of the action occurring in the clinic and must be visible to patients and PCPs alike. Although 80% of patients with unexplained symptoms and psychosocial distress accept manage- ment by PCPs, only 10% will attend a psychosocial referral (Smith et al., 2003). Not having to travel to another facility or even a different area of the clinic to access behavioral health may help reduce the stigma associated with mental illness and thus increase the number of patients receiving services (Pincus, 2003; Strosahl, 1998). Although the concept of a multidisciplinary team is not a new one, redefining the team approach to include PCPs and BHPs requires a willingness to accept a paradigm shift of shared respon- sibility for a patient. A reevaluation of the systems that maintain power differentials among providers at the expense of quality, comprehensive care is necessary, along with efforts to dismantle and rebuild those systems. Using a shared medical record, in which PCPs and BHPs have access to each other’s notes, can help support the paradigm shift. The Health Insurance Portability and Accountability Act (HIPAA)
- 22. regulations clearly delineate the differences between psychother- apy notes and progress notes (Gillman, 2004) and it is the latter kind of note that we suggest BHPs use in integrated settings. Psychotherapy notes are granted special protection under HIPAA due to the likelihood that they contain particularly sensitive infor- mation, are considered the personal notes of the treating therapist, and must be kept separate from the medical record. Progress notes are limited to medication information, modality and frequency of treatment, and a summary of diagnosis, functional status, symp- toms, prognosis, and progress to date. Unlike psychotherapy notes, these notes are part of the medical record. An ideal integrated care system does not operate within a vacuum, but rather allows for coordination of care within and across health care settings. In order to achieve this goal, a service- delivery model must be defined. What patients will be referred out, to whom, and for what reasons? Similarly, what kinds of patients will be accepted from other agencies and for what reasons? In theory, patients with higher mental health needs are better- suited to receive treatment in specialized agencies such as community men- tal health centers (CMHCs). In practice, however, there are sig- nificant barriers to implementing this transition. These obstacles include patients’ reluctance to go to a CMHC because of the
- 23. stigma associated with mental illness, a previous negative experi- ence, long waiting lists, limited transportation options, or failure to meet diagnostic or funding requirements. Moreover, some patients prefer having all health care needs met in one place even when the aforementioned barriers do not apply. Therefore, we argue that an integrated practice that emphasizes primary-care-level behavioral interventions must remain flexible enough to accommodate all patients, regardless of problem severity. Putting It All Together: Salud’s Integrated Care Model There is tremendous variability in the kinds of behavioral health issues seen in our setting, and symptom severity in each patient is fluid rather than static. We argue that behavioral health is not a bimodal phenomenon determined by the presence or absence of health; rather, it exists along a continuum. We conceptualize this continuum as having four levels of severity; at any given time fewer patients fall into the more severe levels and more patients fall into the less severe levels. Conceptualizing our population in this fashion allows us to better allocate resources based on the distribution of patients. Patients presenting at Level 1 are in a state of acute need, requiring immediate referral to emergency departments and/or inpatient care. Examples include imminent suicidal depression,
- 24. acute psychosis, and manic crisis. Because of the seriousness and visible nature of their symptoms, these patients are more likely to present to an emergency room or to be detained by police than they are to present to PCP offices. Level 2 consists of patients who have severe and persistent mental illness. Although these patients can benefit from psychiatric follow-up in a specialized mental health setting, the need is not immediate. Many can be monitored in primary care settings when stable, especially when psychiatry consultation is available. Patients at Level 3 present with problems that are chronic and of lower severity. They are common in primary care practice and include somatization disorders, nonpsy- chotic depression, acute stress disorder, and anxiety disorders where functional impairment is present but the symptoms are not completely debilitating. Level 3 patients frequently seek care in primary care settings, but PCPs are not always equipped with the expertise and knowledge to address their needs (Goldman et al., 2000). Level 4 includes patients with temporary mental health and psychosocial problems, including concerns such as marital diffi - culties, parenting problems, bereavement, employment problems, financial stress, and so forth. Left untreated, Level 4 problems can progress, potentially leading to risky behaviors, unhealthy life choices, and worsening of chronic diseases. Last, at any given time, there are patients who do not qualify for assignment to a particular level but who nevertheless might benefit from educa-
- 25. tional and preventive interventions. In an attempt to provide adequate services to the 80,000 patients in the Salud system in alignment with our mission, we grappled with how BHPs were going to spend their time. We wanted to maximize their ability to see a high number of patients while still maintaining a high standard of care. Based on the four-level model of severity just described, BHPs spend 30% of their time providing more traditional therapy services to Levels 1 and 2, the highest- needs patients, who make up a significant portion, though not the majority of our population. BHPs spend 70% of their time provid- ing various integrated services to Levels 3 and 4 and the unas - signed, whose symptoms are less severe or temporarily nonexistent but who make up a much larger portion of our patient population. After careful consideration, we decided that the best service- delivery model for patients in our geographical area is a stepped- care approach. The initial point of contact with a BHP typically occurs during a medical visit. Of patients requiring follow-up care, some are referred out but many continue with onsite therapy services. Therapy appointments are scheduled separately from medical appointments and consist of a limited number of visits, which can be extended if necessary by department approval. His- torically, referrals to CMHCs more commonly were driven by payer source (i.e., Medicaid) than by patient need, creating a dual
- 26. standard of care whereby some but not all patients received inte- 393ESTABLISHING AN INTEGRATED CARE PRACTICE T hi s do cu m en t i s co py ri gh te d by th e A m er
- 29. p er so na l u se o f t he in di vi du al u se r a nd is n ot to b e
- 30. di ss em in at ed b ro ad ly . grated care. Recently, we have determined that this standard is unacceptable and have made modifications to our care model to allow primarily clinical determinants to inform referral decisions. These clinical determinants include when a patient a) needs ser - vices for a longer period than we can provide; b) requires specialty services such as vocational rehabilitation, day treatment, wrap- around services, and so forth; and c) qualifies as severely and persistently mentally ill or severely emotionally disturbed. Services Offered BHPs at Salud offer a variety of evidence-based services, in- cluding screenings, consultations, psychotherapy, and psycholog- ical assessment. A report by the Institute of Medicine (2001)
- 31. defined evidence-based practice in psychology as the “integration of the best available research with clinical expertise in the context of patient characteristics, culture, and preferences” (p. 147). Re- search suggests that sensitivity and flexibility in administering therapeutic interventions produces better outcomes than rigid ap- plication of manuals or principles (Castonguay, Boswell, Constan- tino, Goldfried, & Hill, 2010; Henry, Schacht, Strupp, Butler, & Binder, 1993; Huppert et al., 2001). Because clinicians with sound clinical judgment will be more effective when operating from treatment perspectives that are most consistent with their views (Benish, Imel, & Wampold, 2008; Luborsky et al., 1999; Wampold, Minami, Baskin, & Tierney, 2002), we encourage BHPs to utilize all of their clinical knowledge from an evidenced- based perspective, rather than limiting themselves to a narrow range of interventions. As opposed to evidence-based practice, empirically validated treatments (EVTs) are specific treatments for defined groups of individuals who have particular disorders. We argue that, although there is certainly a place for EVTs in any setting, applying such interventions in a primary care setting is particularly challenging for several reasons. First, much of the work being done in primary care is brief, which can limit the ability of the BHP to provide the intervention in full-form. Second, the population in primary care is
- 32. extremely heterogeneous. Primary care patients cover the entire life span, present with multiple comorbidities, and do not usually request treatment for a well-defined condition, thus making it extremely difficult to choose the appropriate EVT. Supporting evidence-based practice over EVT makes sense in an integrated primary care setting because it is research-based without being prescriptive. BHPs therefore have latitude to make difficult treat- ment decisions and to derive interventions from the research even when the available research does not fully address the population’s clinical needs (American Psychological Association, 2005). The following section describes Salud’s service-delivery model in greater detail. Screening. The purpose of screening is to identify patients who may be at risk for behavioral health difficulties by detecting previously unrecognized symptoms. Establishing a smooth screen- ing process that does not interrupt the workflow can be challeng- ing. We found that there needs to be clear communication to all employees, including PCPs and support staff, of the expectation that the practice is integrated. Additionally, BHPs and PCPs must have open dialogues about workflow. Last, priority groups need to be established so that BHPs can decide which patients to screen first when it is not possible to screen every patient. Screenings are intended to be structured and brief (5–10 min- utes) and targeted at specific priority groups—for Salud, this includes pregnant patients, postpartum patients, new patients,
- 33. and children. We designed our screenings to encompass conditions specified by the United States Preventive Task Force as well as those concerns commonly seen in our setting. For patients older than 16, we developed an eight-item prescreen the Screen for Life Stressors, containing Yes/No responses about symptoms of de- pression; anxiety; posttraumatic stress disorder (PTSD); tobacco, alcohol, and substance use; and safety in the current living envi - ronment. The questionnaire is a combination of items from the Primary Care Evaluation of Mental Disorders (PRIME-MD), a questionnaire designed to assist general practitioners in the diag- nosis of minor psychiatric disorders (Spitzer et al., 1994); the Primary Care PTSD Screen, a 4-question screen for symptoms of PTSD (Prins et al., 2003); questions based on Screening Brief Intervention Referral to Treatment guidelines for substance use and abuse (Colorado Clinical Guidelines Collaborative, 2008); and questions we developed specifically for this purpose. We typically administer the prescreen face-to-face to help es- tablish a relationship with the patient and to provide the opportu- nity for immediate brief interventions. Positive prescreens trigger a more intensive screening with standardized instruments assess- ing depression, anxiety, alcohol abuse, substance abuse, and PTSD. Depending on the patient’s literacy level, these question- naires can be filled out by the patient or administered interview - style by the BHP. We currently use the following instruments: Patient Health Questionnaire - 9 from the PRIME-MD or Edin- burgh Postnatal Depression Scale (Cox, Holden, & Sagovsky,
- 34. 1987); Generalized Anxiety Disorder (7-item) Scale from the PRIME-MD; PTSD Checklist (Blanchard, Jones-Alexander, Buckley, & Forneris, 1996); Drug Abuse Screening Test (Skinner, 1982); and Alcohol Use Disorders Identification Test (Saunders, Aasland, Babor, de la Fuente, & Grant, 1993). Children are screened using the Parents’ Evaluation of Developmental Status (for ages 0 – 8; Glascoe, 2010) and the Pediatric Symptom Check- list (for ages 9 –16; Jellinek, Murphy, & Burns, 1986). Because false positives are inherent in any screening procedure, formal diagnoses are not based solely on the results of a screening. Screenings that turn into diagnostic assessments are documented separately. When patients screen positive, the BHP or PCP offers follow-up services, either onsite, if possible, or through an outside agency (Pignone et al., 2002). Consultation. Although BHPs can see any patient at any time for any reason, PCPs will often ask a BHP to evaluate and/or treat a patient during a medical visit. Reasons for requesting consulta- tion include but are not limited to psychoeducation or therapeutic interventions for a specific behavioral health concern, health be- havior change interventions, and assessment for diagnostic impres- sions, suicide risk, and capacity to make health care decisions. PCPs also frequently request crisis management services and/or referral for onsite or offsite services.
- 35. Psychotherapy. Full time BHPs have the ability to schedule up to three patients per day for individual psychotherapy appoint- ments. Patients seen in this capacity complete disclosure and informed-consent forms and work with their BHP to develop a treatment plan. The typical session length is 50 minutes, although some clinicians prefer shorter intervals. Scheduling is done either by the BHP directly or through a centralized call center. Given the 394 AUXIER, FARLEY, AND SEIFERT T hi s do cu m en t i s co py ri gh te d
- 38. ol el y fo r t he p er so na l u se o f t he in di vi du al u se r a nd
- 39. is n ot to b e di ss em in at ed b ro ad ly . nature of a primary care setting, termination for no-shows/ cancellations is determined on a case-by-case basis. BHPs need to be flexible when scheduling patients as many will not fall into the traditional once per week model. Psychological testing. Psychological testing for adults is
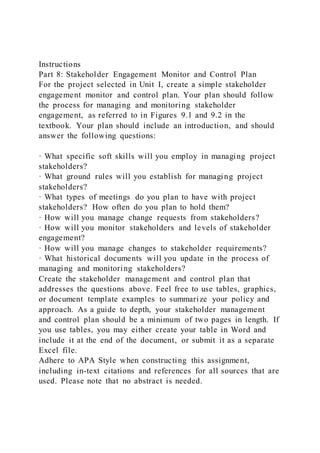
- 40. provided through Salud’s psychology training program, which includes six postdoctoral fellows and several graduate-level practi- cum trainees. A licensed psychologist on staff provides supervi - sion to any trainee completing testing. Reasons for testing include diagnostic clarification to inform medication management and psychotherapy, to rule out a learning disorder, to evaluate memory (e.g., normal aging vs. abnormal memory functioning; specify type of memory impairment), to determine need for intensive neuro- psychological testing, and to assess intellectual functioning. Patient Contacts Using the reporting functions from our electronic health record and billing system, we were able to capture the number of patients seen in 2010. Table 1 shows the results of the prescreenings described above. Table 2 reflects the other behavioral health ser- vices rendered in 2010. The behavioral health team provided approximately 3000 screenings, 5500 consults, and 1800 individ- ual therapy visits in 2010. Financing In a health care system characterized by barriers to integrated practice, especially financial ones, it is surprising that so many practices are making the move toward integration. We think inte- gration is essential for comprehensive patient care consistent with a patient-centered philosophy, but cost-effectiveness is hard to
- 41. measure. Higher levels of integration are more costly due to the staffing and administrative demands associated with more com- plex service delivery. Integration reduces costs for the entire health care system to a point (Chiles et al., 1999; Katon et al., 2006; Mumford, Schlesinger, Glass, Patrick, & Cuerdon, 1984), but primary care practices may not share directly in the cost savings from effectiveness. From a strict revenue-producing standpoint, Salud’s integrated care team does not generate enough revenue to support its staffing. Nevertheless, the cost of funding integration must be compared to the cost of not funding integration. As a federally qualified health center, Salud receives 20% of its $50 million/year operating budget from the federal government, 20% from state grants, and 60% from direct patient fees. Enhanced Medicaid reimbursements for medical visits help offset the costs of providing services to such a large percentage of uninsured indi - viduals. Federally qualified health centers cannot receive any additional reimbursement from Medicaid for behavioral health services during medical visits because the Medicaid rate is a flat per-patient rate regardless of the number or type of services rendered during a particular visit. It is possible to bill Medicaid for services outside a regular medical visit by contracting with the behavioral health organizations that administer Medicaid. How - ever, for the time being, we have chosen not to pursue this funding stream because the current regulations are not favorable to i nte- grated systems. Salud generates a small amount of revenue through
- 42. direct patient fees for therapy and assessment services rendered to non-Medicaid patients. Third-party payers are not billed because of paneling and credentialing requirements for provi ders, same- day billing restrictions, administrative burden, and internal costs associated with electronic claims. We thus decided to pursue other funding for our integrated program. The behavioral health program remains viable through two ongoing Health Resources Services Administration (HRSA) grants, included in Salud’s annual HRSA funding for operating as a federally qualified health center. The psychology training pro- gram is sustained through a combination of grants, including a large one dedicated specifically to postdoctoral training. Finally, many of our BHPs are employed through collaborative arrange- ments with our CMHC partners or similar agencies. In these cases, Salud does not pay the BHP’s salary; the outside agencies benefit by increasing their Medicaid penetration rate and/or by demon- strating that they are reaching more patients. Conclusion Primary care patients who have behavioral health problems are very expensive to the system (Petterson et al., 2008), and behav- ioral health affects overall health whether we address it or not. This Table 1
- 43. Prescreening Results 2010 Dimension Positive screen Negative screen Total % Positive Depression 1066 1924 2990 35.7 Anxiety 979 1865 2844 34.4 Trauma 338 2549 2887 11.7 Alcohol 302 2689 2991 10.1 Tobacco Use 879 1551 2430 36.2 Other Substance Abuse 105 2319 2424 4.3 Unsafe Living Environment 59 2845 2904 2 Table 2 Other Behavioral Health Contacts, 2010 Service Number of contacts Consultation 5507 Diagnostic Evaluations 310 Individual therapy 1844 Family therapy 82 Group therapy 37 Smoking cessation 237 Alcohol/Substance Treatment 73 Child Screen 299 395ESTABLISHING AN INTEGRATED CARE PRACTICE T hi s do cu m
- 48. ly . article has been an attempt to describe how these basic consider- ations have driven the evolution of an integrated care practice in a large community health center system that serves vulnerable pop- ulations across North Central Colorado. With the caveat that there is no one correct way to achieve integrated care, we have presented the various considerations and decisions made along the way in hopes that others who are considering or are in the process of establishing an integrated care practice might learn from our experiences. We have detailed our thoughts about the necessary and sufficient components of successful integration, with special attention to the role of evidence-based practice. We have also argued that paradigm shifts from a medically focused mentality to a patient-centered mentality must be made at the organizational level. For practices considering integrating behavioral health into pri - mary care, is value measured by dollars brought into the organi - zation, provider satisfaction, patient satisfaction, decreased utili- zation, fewer emergency room visits, or improvement in physical markers? If the only way to generate revenue through behavioral
- 49. health services is by moving from an integrated to a colocated model, is this approach consistent with the organizational mission? Do the administrative burdens and costs of billing fee-for- service outweigh the benefits? Do they impact the organization’s ability to offer high-volume quality services? These are merely a few of the questions that will arise when setting up an integrated care prac- tice. References Adashi, E. Y., Geiger, H. J., & Fine, M. D. (2010). Health care reform and primary care–the growing importance of the community health center. The New England Journal of Medicine, 362, 2047–2050. doi:10.1056/ NEJMp1003729 Agency for Healthcare Research and Quality. (2008). Total expenses and percent distribution for selected conditions by type of service: United States, 2008. Medical Expenditure Panel Survey Household Component Data. Retrieved from http://www.meps.ahrq.gov/mepsweb/data_stats/ tables_compendia_hh_interactive.jsp?_SERVICE�MEPSSocket 0&_ PROGRAM � MEPSPGM. TC. SAS & File � HCFY2008 & Table � HCFY2008%5FCNDXP%5FC&_Debug�
- 50. American Psychological Association. (2005). Report of the 2005 presiden- tial task force on evidence-based practice. Retrieved from http:// www.apa.org/practice/resources/evidence/evidence-based- report.pdf Benish, S. G., Imel, Z. E., & Wampold, B. E. (2008). The relative efficacy of bona fide psychotherapies for treating post-traumatic stress disorder: A meta-analysis of direct comparisons. Clinical Psychology Review, 28, 746 –758. doi:10.1016/j.cpr.2007.10.005 Blanchard, E. B., Jones-Alexander, J., Buckley, T. C., & Forneris, C. A. (1996). Psychometric properties of the PTSD Checklist (PCL). Behav- iour Research and Therapy, 34, 669 – 673. doi:10.1016/0005- 7967(96)00033-2 Blount, A. (2003). Integrated primary care: Organizing the evidence. Families, Systems, & Health, 21, 121–133. doi:10.1037/1091- 7527.21.2.121 Butler, M., Kane, R. L., McAlpin, D., Kathol, R. G., Fu, S. S., Hagedorn, H., & Wilt, T. J. (2008). Integration of mental health/substance abuse and primary care No. 173 (AHRQ Publication No. 09-E003). Rockville, MD: Agency for Healthcare Research and Quality.
- 51. Castonguay, L. G., Boswell, J. F., Constantino, M. J., Goldfried, M. R., & Hill, C. E. (2010). Training implications of harmful effects of psycho- logical treatments. The American Psychologist, 65, 34 – 49. doi:10.1037/ a0017330 Chiles, J. A., Lambert, M. J., & Hatch, A. L. (1999). The impact of psychological interventions on medical cost offset: A meta- analytic review. Clinical Psychology: Science and practice, 6, 204 –220. doi: 10.1093/clipsy.6.2.204 Colorado Clinical Guidelines Collaborative. (2008). Guideline for alcohol and substance use screening, brief intervention, referral to treatment. Retrieved from http://www.healthteamworks.org/guidelines/sbirt.html Cox, J. L., Holden, J. M., & Sagovsky, R. (1987). Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depres- sion Scale. British Journal of Psychiatry, 150, 782–786. doi:10.1192/ bjp.150.6.782 Cwikel, J. Zilber, N. Feinson. M., & Lerner, Y. (2008). Prevalence and risk factors of threshold and sub-threshold psychiatric disorders in primary care. Social Psychiatry and Psychiatric Epidemiology, 43, 184 –
- 52. 191. doi:10.1007/s00127-007-0286-9 Gillman, P. B. (2004). A new era of documentation in psychiatry: Advice on psychotherapy, progress notes. Behavioral Healthcare Tomorrow, 13, 48 –50. Glascoe, F. P. (2010). Parents’ Evaluation of Developmental Status (PEDS). Nolensville, TN: PEDSTest.com, LLC. Goldman, H. H., Rye, P., & Sirovatka, P. (2000). A report of the surgeon general. Washington, DC: Department of Health and Human Services. Henry, W. P., Schacht, T. E., Strupp, H. H., Butler, S. F., & Binder, J. L. (1993). Effects of training in time-limited dynamic psychotherapy: Changes in therapist behavior. Journal of Consulting and Clinical Psy- chology, 61, 434 – 440. doi:10.1037/0022-006X.61.3.434 Huppert, J. D., Bufka, L. F., Barlow, D. H., Gorman, J. M., Shear, M. K., & Woods, S. W. (2001). Therapist, therapist variables, and cognitive- behavioral therapy outcomes in a multicenter trial for pani c disorder. Journal of Consulting and Clinical Psychology, 69, 747–755. doi: 10.1037/0022-006X.69.5.747
- 53. Ibrahim, M., Savitz, L., Carey, T., & Wagner, E. (2001). Population-based health principles in medical and public health practice. Journal of Public Health Management, 7, 75– 81. Institute of Medicine. (2001). Crossing the quality chasm: A new health system for the 21st Century. Washington, DC: National Academies Press. Retrieved from http://www.nap.edu/catalog.php?recor - d_id�10027 Institute of Medicine. (2006). Improving the quality of healthcare for mental and substance-use conditions: Quality chasm series. Washing- ton, DC: National Academies Press. Retrieved from http://www .nap.edu/catalog.php?record_id�11470#toc Jellinek, M. S., Murphy, J. M., & Burns, B. J. (1986). Brief psychosocial screening in outpatient pediatric practice. Journal of Pediatrics, 109, 371–378. doi:10.1016/S0022-3476(86)80408-5 Katon, W. J., Unutzer, J., Fan, M., Williams, J. W., Schoenbaum, M., Lin, E. H., & Hunkeler, E. M. (2006). Cost-effectiveness and net benefit of enhanced treatment of depression for older adults with diabetes and depression. Diabetes Care, 29, 265–270. doi:10.2337/diacare .29.02.06.dc05–1572 Klinkman, M. S. (2009). Assessing functional outcomes in
- 54. clinical prac- tice. The American Journal of Managed Care, 15, S335–S342. Luborsky, L., Diguer, L., Seligman, D. A., Rosenthal, R., Krause, E. D., Johnson, S., . . . Schweizer, E. (1999). The researcher’s own therapeutic allegiances: A “wild card” in comparisons of treatment efficacy. Clinical Psychology: Science and Practice, 6, 95–106. doi:10.1093/clipsy/6.1.95 McGinnis, J. M., & Foege, W. H. (1993). Actual causes of death in the United States. Journal of the American Medical Association, 270, 2207– 2212. doi:10.1001/jama.270.18.2207 Mokdad, A. H., Marks, J. S., Stroup, D. F., & Gerberding, J. L. (2004). Actual causes of death in the United States, 2000. Journal of the American Medical Association, 291, 1230 –1245. doi:10.1001/ jama.291.10.1238 Mumford, E., Schlesinger, H. J., Glass, G. V., Patrick, C., & Cuerdon, T. 396 AUXIER, FARLEY, AND SEIFERT T hi s do cu
- 59. ad ly . (1984). A new look at evidence about reduced cost of medical utilization following mental health treatment. American Journal of Psychiatry, 141, 1145–1158. O’Donohue, W. T., Cummings, N. A., & Ferguson, K. E. (2003). Clinical integration: The promise and the path. In N. A. Cummings, W. T. O’Donohue, & K. E. Ferguson (Eds.), Behavioral health as primary care: Beyond efficacy to effectiveness (pp. 15–30). Reno, NV: Context. Petterson, S. M., Phillips, R. L., Bazemore, A. W., Dodoo, M. S., Zhang, X., & Green, L. A. (2008). Why there must be room for mental health in the medical home. American Family Physicians, 77, 757. Pignone, M. P., Gaynes, B. N., Rushton, J. L., Burchell, C. M., Orleans, C. T., Mulrow, C. D., & Lohr, K. N. (2002). Screening for depression in adults: A summary of the evidence for the U.S. Preventive Services Task Force. Annals of Internal Medicine, 136, 765–776.
- 60. Pincus, H. A. (2003). The future of behavioral health and primary care: Drowning in the mainstream or left on the bank? Psychosomatics, 44, 1–11. doi:10.1176/appi.psy.44.1.1 Prins, A., Ouimette, P., Kimerling, R., Cameron, R. P., Hugelshofer, D. S., Shaw-Hegwer, J., . . . Sheikh, J. I. (2003). The primary care PTSD screen (PC-PTSD): Development and operating characteristics. Primary Care Psychiatry, 9, 9 –14. doi:10.1185/135525703125002360 Rabin, D., Petterson, S. M., Bazemore, A. W., Teevan, B., Phillips, R. L., Dodoo, M. S., & Xierali, I. (2009). Decreasing self-perceived health status despite rising health expenditures. American Family Physician, 80, 427. Saunders, J. B., Aasland, O. G., Babor, T. F., de la Fuente, J. R., & Grant, M. (1993). Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption. II. Addiction, 88, 791– 804. doi: 10.1111/j.1360-0443.1993.tb02093.x Skinner, H. A. (1982). The Drug Abuse Screening Test. Addictive Behav- ior, 7, 363–371. doi:10.1016/0306-4603(82)90005-3
- 61. Smith, R. C., Lein, C., Collins, C., Lyles, J. S., Given, B., Dwamena, F. C., . . . Given, C. W. (2003). Treating patients with medically unexplained symptoms in primary care. Journal of General Internal Medicine, 18, 478 – 489. doi:10.1046/j.1525-1497.2003.20815.x Spitzer, R. L., Williams, J. B., Kroenke, K., Linzer, M., deGruy, F. V., Hahn, S. R., . . . Johnson, J. G. (1994). Utility of a new procedure for diagnosing mental disorders in primary care: The PRIME-MD 1000 Study. Journal of the American Medical Association, 272, 1749 –1756. doi:10.1001/jama.272.22.1749 Strosahl, K. (1998). Integrated primary care behavioral health services: The primary mental healthcare paradigm. In A. Blount (Ed.), Integrative primary care: The future of medical and mental health collaboration (pp. 139 –166). New York: Norton. U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration. (2006). Transforming mental healthcare in America: The federal action agenda: First steps. Retrieved from http://www.samhsa.gov/Federalactionagenda/NFC_execsum.asp x
- 62. Wampold, B. E., Minami, T., Baskin, T., & Tierney, S. (2002). A meta- (re)analysis of the effects of cognitive therapy versus “other therapies” for depression. Journal of Affective Disorders, 68, 159 –165. doi: 10.1016/S0165-0327(00)00287-1 Wang, P. S., Demler, O., Olfson, M., Pincus, H. A., Wells, K. B., & Kessler, R. C. (2006). Changing profiles of service sectors used for mental healthcare in the United States. American Journal of Psychiatry, 163, 1187–1198. doi:10.1176/appi.ajp.163.7.1187 World Health Organization & World Organization of Family Doctors. (2008). Integrating mental health into primary care: A global perspec- tive. Geneva: World Health Organization. Retrieved from http:// whqlibdoc.who.int/publications/2008/9789241563680_eng.pdf Received March 21, 2011 Revision received June 9, 2011 Accepted June 15, 2011 � 397ESTABLISHING AN INTEGRATED CARE PRACTICE T hi s do
- 67. ro ad ly . Integrating Behavioral Health Services Into a University Health Center: Patient and Provider Satisfaction Jennifer S. Funderburk, PhD VA Center for Integrated Healthcare, Syracuse, New York, Syracuse University, and University of Rochester Robyn L. Fielder, MS Syracuse University Kelly S. DeMartini, PhD Syracuse University and Yale University School of Medicine Cheryl A. Flynn, MD University of Vermont The goals of this study were to (a) describe an Integrated Behavioral Health Care (IBHC) program within a university health center and (b) assess provider and patient acceptability and satisfaction with the IBHC program, including
- 68. behavioral health screening and clinical services of integrated behavioral health providers (BHPs). Fifteen providers (nine primary care providers and six nurses) and 79 patients (75% female, 65% Caucasian) completed program ratings in 2010. Providers completed an anonymous web-based questionnaire that assessed satisfaction with and acceptability of behavioral health screening and the IBHC program featuring integrated BHPs. Patients completed an anonymous web-based questionnaire that assessed program satisfaction and comfort with BHPs. Providers reported that behavioral health screening stimulated new conversations about behavioral health concerns, the BHPs provided clinically useful services, and patients benefited from the IBHC program. Patients reported satisfaction with behavioral health services and reported a willingness to meet again with BHPs. Providers and patients found the IBHC program beneficial to clinical care. Use of integrated BHPs can help university health centers support regular screening for mental and behavioral health issues. Care integration increases access to needed mental health treatment. Keywords: integrated behavioral health care, integrated primary care, mental health care Integrated behavioral health care (IBHC), in which primary care providers (PCPs) and be- havioral health providers (BHPs) collaborate to provide coordinated care, is an emerging model
- 69. of patient care. Over the past decade, research has identified IBHC as a clinically effective and cost-effective method for improving clinical outcomes within primary care settings (Blount et al., 2007; Bryan, Morrow, & Appolonio, 2009; Cigrang, Dobmeyer, Becknell, Roa- Navarrete, & Yerian, 2006; Goodie, Isler, Hun- ger, & Peterson, 2009). Typically, this research has focused on integrating mental and behav- ioral health care within adult primary care set- This article was published Online First May 21, 2012. Jennifer S. Funderburk, PhD, VA Center for Integrated Healthcare, Syracuse, New York, Department of Psychol- ogy, Syracuse University, and Department of Psychiatry, University of Rochester; Robyn L. Fielder, MS, Depart- ment of Psychology, Syracuse University; Kelly S. DeMar- tini, PhD, Department of Psychology, Syracuse University and Department of Psychiatry, Yale University School of Medicine; Cheryl A. Flynn, MD, Center for Health and Wellbeing, University of Vermont. The views expressed in this article are those of the authors and do not reflect the official policy of the Veterans’ Affairs’ depart- ment or other departments of the U.S. government. This material is based upon work supported by the American College Health Association United Healthcare Student Recourse Initiatives in College Mental and Behavioral Health grant. Correspondence concerning this article should be ad- dressed to Jennifer S. Funderburk, Center for Integrated Healthcare, 800 Irving Avenue, Room 116C, Syracuse,
- 70. NY 13210. E-mail: [email protected] Families, Systems, & Health © 2012 American Psychological Association 2012, Vol. 30, No. 2, 130 –140 1091-7527/12/$12.00 DOI: 10.1037/a0028378 130 T hi s do cu m en t i s co py ri gh te d by th e A
- 73. r t he p er so na l u se o f t he in di vi du al u se r a nd is n ot to
- 74. b e di ss em in at ed b ro ad ly . tings, such as private family medicine practices, academic medical center primary care clinics, and primary care services offered within the Veterans Health Administration or Federal Qualified Centers. However, there is little re- search examining IBHC in university health clinics. University health centers share many features with standard primary care settings. For exam- ple, university health centers tend to offer am- bulatory care and other basic medical services to a wide range of patients (Christmas, 1995). These clinics tend to be students’ first option
- 75. when seeking medical care in nonemergency situations. University health centers may coor- dinate referrals to off-campus specialists as nec- essary. Thus, in terms of services offered and general approach to care, university health cen- ters and primary care clinics are quite similar. Nevertheless, compared with typical primary care practices, university health clinics are somewhat unique in that they generally serve a restricted age range (i.e., 18 –24 years of age) for a limited period of time (i.e., academic se- mesters) that has predictable elevations in stress/illness as a result of the increased work- load that occurs toward the end of the semester. In addition, a majority of students are develop- mentally just beginning to take care of them- selves while continuing to maintain significant ties to their parents, sometimes limiting their financial resources and ability to travel off cam- pus for additional specialty services. Another caveat is that most university health clinics pro- vide services to students using a general health fee that is wrapped into their tuition, eliminating difficulties with insurance claims (Mills, Gold, & Curran, 1996). The lack of research examining the integra- tion of mental health services into university health clinics is surprising because of the alarm- ing rates of mental health issues on college campuses (American College Health Associa- tion [ACHA], 2010a; Mowbray et al., 2006) and the fact that most college students with clini- cally significant psychological distress do not receive mental health treatment (Rosenthal & Wilson, 2008). For instance, only 15% of stu-
- 76. dents with moderately severe to severe depres- sion or past-month suicidal ideation received any mental health care (Garlow et al., 2008). A recent ACHA white paper (2010b) argued for the integration of campus medical and counsel- ing clinics, given the great potential for inte- grated care to increase treatment access, en- hance clinical outcomes, and improve patient satisfaction. Similar to other primary care settings, IBHC in university health centers can provide an av- enue to address many of the obstacles to treat- ment access for college students. For instance, a higher proportion of students use campus health clinics than campus mental health clinics (79% vs. 10% in one recent study; Eisenberg, Golber- stein & Gollust, 2007), and many students feel more comfortable seeing PCPs than therapists (ACHA, 2010b). Moreover, because many mental health issues cause physical symptoms, many students seek evaluation at health clinics first (ACHA, 2010b). The few studies examin- ing IBHC within university health settings have reported numerous benefits, including increased accessibility of mental/behavioral health care, increased referral follow-through, and higher quality patient care (Masters, Stillman, Brown- ing & Davis, 2005; Tucker, Sloan, Vance, & Brownson, 2008; Westheimer & Steinley- Bumgarner, 2008). Besides clinical outcomes, another vital com- ponent in the process of evaluating a new program of service, and whether others should
- 77. consider implementing such a program within college health, is obtaining feedback from the “consumers” involved in the program (Gallo et al., 2004; Reiss-Brennan, Briot, Daumit, & Ford, 2006; Runyan, Fonseca, & Hunter, 2003). For IBHC, primary consumers include PCPs and patients. A lack of acceptability and/or sat- isfaction among the PCPs with the various com- ponents of the IBHC program would ultimately sabotage the program because of (a) the pivotal role PCPs have within IBHC (i.e., referring patients to BHPs) and (b) the focus all IBHC programs have on increasing collaboration be- tween PCPs and BHPs. Similarly, it is ex- tremely important that the patients are satisfied with clinical services provided by a new program, otherwise patients may not remain engaged or comply with treatment recommen- dations, which could compromise treatment success. Patient satisfaction is an important out- come measure that identifies problems with health care (Sitzia & Wood, 1997) and is asso- ciated with treatment adherence and provider/ program selection (Fitzpatrick, 1991). 131INTEGRATING BEHAVIORAL HEALTH SERVICES T hi s do cu m
- 82. ly . Preliminary studies have begun to examine patient and provider opinions about IBHC within the college health setting. Tucker et al. (2008) examined an international student’s ex- perience of the Integrated Health Program at the University of Texas at Austin using a case study design and found his overall experience to be positive. Westheimer and Steinley-Bumgarner (2008) examined provider behaviors, opinions, and experiences during the integration process of IBHC within the same university and found PCPs ascribed a high level of value to the col- laborative effort integrated BHPs could provide in helping with a diverse number of conditions. However, neither of these studies provided a sound understanding of patient or provider sat- isfaction with the IBHC program and its various components. Two studies have examined the use of screen- ing questionnaires designed to increase discus- sion of mental and behavioral health issues dur- ing university health center visits. In a pilot study, Cowan and Morewitz (1995) found that use of a screening questionnaire prompted dis- cussion of psychosocial concerns that may not have otherwise come up. However, this study did not use a validated screening measure or examine provider or patient satisfaction with use of the screening measure. Alschuler, Hoodin, and Byrd (2008) examined provider
- 83. and patient satisfaction with the integration of a screening questionnaire for behavioral health issues in a college health center. They found that patients who were randomly assigned to fill out the screening questionnaire reported it helped them discuss concerns with their provid- ers and they would like its use to continue in the future. The providers reported that they also found the screening questionnaire helpful and would be happy to collaborate with integrated BHPs on-site. Although this study provided pre- liminary evidence toward patient and provider satisfaction with IBHC, it focused on integrat- ing the screening measure and it did not involve the actual integration of BHPs, which is a fun- damental component of IBHC programs. In sum, IBHC is an emerging approach to health care that can increase access to mental and behavioral health care while reducing the burden on PCPs and specialty mental health centers. University health centers are an oppor- tune setting in which to implement the IBHC model. However, despite the importance of en- suring provider and patient acceptability and satisfaction when implementing new clinical programs, little research has examined these factors with respect to IBHC in university health centers. Therefore, the purpose of this study was to collect feedback from PCPs and patients to assess the acceptability and satisfac- tion with all aspects of integrating an IBHC program at Syracuse University, which included the implementation of a behavioral health screening questionnaire as well as the integra-
- 84. tion of several BHPs. It was expected that PCPs and patients would indicate a high level of sat- isfaction and acceptability with all aspects of the program. Method Our Integrated Behavioral Health Primary Care Program We developed our IBHC program by adapt- ing a common model of integrated health care called the Primary Mental Health Care model described by Strosahl (1998). Syracuse Univer- sity Health Services (SUHS), which serves ap- proximately 9,038 patients per year, collabo- rated with the Syracuse University doctoral program in clinical psychology to integrate three to five advanced doctoral students as BHPs per academic year (for additional infor- mation regarding this type of collaborative ef- fort, see Masters et al., 2005). The BHPs pro- vided clinical services 20 –35 hours per week as part of an Advanced Practicum course. Working under the supervision of a licensed psychologist and an onsite medical provider, the BHPs saw approximately 152 students per semester for various presenting problems (e.g., insomnia, de- pressive symptoms). BHPs acted as consultants to the PCPs, seeing patients for brief sessions (i.e., one to three sessions lasting approximately 15–30 minutes each; Strosahl, 1998). The aver- age number of sessions per patient was 1.43 (SD � 0.83, range 1–5) for the Spring, 2010 semester and 1.61 (SD � 0.97, range 1– 6) for the Fall, 2010 semester.
- 85. In this IBHC model, the PCP ultimately maintains responsibility for patient manage- ment throughout the course of treatment. None- theless, the PCPs can utilize the BHPs in several ways: (a) to conduct further assessment of be- havioral health issues; (b) to provide brief in- 132 FUNDERBURK, FIELDER, DEMARTINI, AND FLYNN T hi s do cu m en t i s co py ri gh te d by th e
- 88. fo r t he p er so na l u se o f t he in di vi du al u se r a nd is n ot
- 89. to b e di ss em in at ed b ro ad ly . terventions for patients reporting mild-moderate mental health symptomatology, behavioral health issues (e.g., sleep problems), or symp- toms associated with chronic disease; (c) to triage patients reporting more severe mental health symptoms to more specialized services; and (d) to provide crisis assessment. BHPs maintain an open access schedule, keeping at least 15 minutes free between half-hour ap- pointments to allow PCPs to walk patients down for same-day visits. Assessments and pa- tient progress notes are shared among the team
- 90. via verbal and/or written communications within the electronic medical record. Therefore, this IBHC model is strikingly different from the colocation of specialty mental health services within a university health clinic, which often continues to maintain separate medical records, provide more intensive treatment (i.e., a higher number of sessions, longer sessions), see pa- tients for more severe symptomatology, and is often unable to accommodate same-day noncri- sis appointments. To help facilitate referrals and to follow na- tional recommendations regarding screening for depression and at-risk alcohol use among young adults (American Academy of Pediatrics, 2001; Nimalasuriya, Compton, Guillory & Prevention Practice Committee of the American College of Preventive Medicine, 2009; U.S. Preventive Services Task Force, 2009), we implemented a screening tool as part of our IBHC program. Specifically, all students seen by PCPs for any reason were screened for the following symp- toms: (a) depression and suicidal ideation with the Patient Health Questionnaire-9 (PHQ-9; Spitzer, Kroenke & Williams, 1999); (b) at-risk alcohol use with the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C; Saunders, Aasland, Babor, de la Fuente & Grant, 1993); (c) sleep problems with two items from the Insomnia Severity Index (ISI; Bastien, Valliéres & Morin, 2002); and (d) tobacco use with three items to assess smoking habits. Stu- dents were given the screening tool by nurses as they waited for the medical providers follow - ing the nurse obtaining vital signs. The screen-
- 91. ing tool clearly describes the purpose of the questionnaire, the confidentiality of the infor- mation, and that the items ask about symptoms unrelated to any current acute illness (e.g., cold, flu). Procedure This study was approved by the Syracuse University Institutional Review Board. To ob- tain the provider satisfaction data, we sent three recruitment emails, one week apart, to all PCPs and nurses working at the university health clinic over a 4-week period during the Spring semester of 2010. The email provided a brief description of the study and linked the provider to an anonymous web-based questionnaire. Af- ter providing informed consent, participants provided information on whether they were a PCP (MD, NP) or nurse and filled out a provider satisfaction survey. Providers were not given any compensation for participation. To obtain the patient satisfaction data, we obtained a list of all students who had at least one session with an integrated BHP during the Spring (i.e., January 15 to May 15, 2010) or Fall semester in 2010 (i.e., August 15 to Decem- ber 15, 2010) by pulling a list of all patients who were included in the electronic medical record as having the specific encounter code used only by the BHPs to identify behavioral health visits. Then, email addresses were lo- cated using the publicly available student email address directory. In addition, basic demo- graphics of all IBHC patients were obtained
- 92. from a tracking database maintained by the BHPs. We sent three recruitment emails, ap- proximately 3– 4 weeks apart, to each identified patient at the end of each semester to their university-provided email address to ask them to participate in an anonymous web-based pa- tient satisfaction survey. After completing in- formed consent, participants completed the questionnaire. As an incentive, participants were offered a chance to win one of 12 $25 gift cards to an online retailer. Participants All PCPs (n � 9, two physician and seven nurse practitioners) and nurses (n � 10) work- ing in the university health clinic were eligible to complete the provider satisfaction question- naire. Fifteen participants (nine PCPs and six nurses) did so, yielding a 79% (100% for PCPs and 60% for nurses) response rate. Because of the small number of providers at the clinic and the need to maintain their anonymity to encour- age higher response rates and candid respond- 133INTEGRATING BEHAVIORAL HEALTH SERVICES T hi s do cu m
- 97. ly . ing, we did not collect demographics from the participants. A total of 303 (175 Spring semester, 128 Fall semester) unique IBHC patients were identified using the electronic medical record. A total of 27 (23 from Spring semester and four from Fall semester) had recruitment emails returned because of a nonexistent address error likely resulting from the fact that the student left the university for some reason (e.g., graduation). Of the remaining participants who were eligible (n � 276), 79 participants (32 Spring semes- ter, 47 Fall semester) completed the patient sat- isfaction survey, resulting in an overall 29% response rate (n � 152, 21% for Spring semes- ter and n � 124, 38% for Fall semester). The majority of the participants were female (n � 59, 75%), white (n � 51, 65%), and not Hispanic or Latino (n � 72, 91%). To under- stand the representativeness of our sample, Table 1 presents the demographics for those who partic- ipated in the study and for the total sample of patients (n � 303) who saw a BHP during the Spring and Fall semesters of 2010. Because the patient satisfaction survey was anonymous, we were unable to test for demographic differences between responders and nonresponders. Measures
- 98. Provider satisfaction questionnaire. Par- ticipants rated their level of agreement with 18 statements about the acceptability and useful- ness of each component of the IBHC program on a Likert scale that ranged from strongly disagree (1) to neutral (3) to strongly agree (5). The 18 items (see Table 2) were generated by the first and fourth author and focused on each element of the IBHC program implemented. For several items, the participant could choose “not applicable” because of the lack of relevance of the statement to nurses versus PCPs and vice versa. Cronbach’s alpha for the scale was .80. Patient satisfaction questionnaire. Par- ticipants answered five demographic questions (i.e., age, sex, race, ethnicity, and class in school), and three yes/no questions (i.e., whether they remembered filling out the screen- ing measure, whether their PCP discussed one of the topics on the screening measure with them, and whether they met with an integrated BHP). Those who remembered filling out the screening measure and meeting with the inte- grated BHP completed an additional six state- ments (see Table 3) which asked participants to rate their level of satisfaction, comfort, or will- ingness on a Likert scale that ranged from (1) extremely unsatisfied/uncomfortable/unwilling to (3) neutral to (5) extremely satisfied/ comfortable/willing on a variety of elements associated with the IBHC program. These items were generated by the first and fourth author. For those participants who completed the Likert portion of the questionnaire, Cronbach’s alpha
- 99. for those six items was .75. Table 1 Demographics of Survey Participants and All IBHC Patients Participant Demographics All IBHC Patients M SD n % M SD n % Age 30.0 3.8 79 21.7 4.1 303 Males 20 25.3 121 40.0 Hispanic or Latino 7 8.9 22 7.3 Racea White 51 64.6 201 66.3 Black 7 8.9 34 11.2 Asian 10 12.7 24 7.9 Other 10 12.7 44 14.5 Classb Freshman 4 5.1 55 18.2 Sophomore 22 27.8 55 18.2 Junior 17 21.5 47 15.5 Senior 9 11.4 67 22.1 Graduate Student 27 34.2 75 24.8 a One participant left race unknown. b Four patients’ class was unknown. 134 FUNDERBURK, FIELDER, DEMARTINI, AND FLYNN T hi s
- 104. b ro ad ly . Data Analytic Plan Because of the descriptive nature of the ob- jectives of this study, our data analytic plan focused primarily on examining distributions and calculating the frequencies, modes, means, and standard deviations of individual survey items. Results Provider Satisfaction As shown in Table 2, both PCPs and nurses reported a high level of support for regular implementation of the screening measure across all four screening domains and reported that patients were comfortable answering the ques- tions on the screening measure. Providers strongly agreed that the screening measure helped stimulate discussion on topics that would not have come up during the visit other- wise. There was a greater level of variability yielding average (i.e., means ranging from 2.5– 3.0) and modal responses within the neutral
- 105. range for the two items assessing whether the screening measure took too much time away from other clinical duties and was difficult to score and interpret. PCPs and nurses considered the integrated BHPs a part of the primary care team and felt the IBHC program helped patients receive treat- ment more quickly. PCPs perceived that pa- Table 2 Provider Ratings of IBHC Acceptability and Satisfaction Item PCPs Nurses n M (SD) Range n M (SD) Range Rate your level of agreement with the implementation of regular screening at SUHS for a) Depression 9 4.7 (0.5) 4–5 6 4.7 (0.5) 4–5 b) Sleep problems 9 4.3 (1.0) 2–5 6 4.7 (0.5) 4–5 c) Tobacco use 9 4.2 (0.7) 3–5 6 4.6 (0.5) 4–5 d) Alcohol misuse 9 4.7 (0.5) 4–5 6 4.7 (0.5) 4–5 The items that assessed the problem below were useful in my clinical practice a) Depressed mood 9 4.4 (0.5) 4–5 2 4.0 (1.4) 3–5 b) Sleep problems 9 3.9 (0.9) 2–5 1 5.0 (0.0) 5 c) Tobacco use 9 3.4 (0.7) 3–5 1 5.0 (0.0) 5 d) Alcohol consumption 9 3.8 (1.0) 2–5 2 4.5 (0.7) 4–5
- 106. The screening measure Took too much time away from clinical duties 9 2.9 (0.8) 2–4 6 2.5 (0.8) 1–3 Was difficult to score and interpret 9 2.6 (1.2) 1–4 5 3.0 (0.7) 2–4 Helped stimulate discussion of topics that would not have come up during patient visits 9 4.3 (0.7) 3–5 1 5.0 (0.0) 5 A majority of my patients felt comfortable answering the questions on the screening measure 9 4.3 (1.0) 2–5 6 3.8 (0.8) 3–5 The BHPs Were useful within my clinical practice 9 4.7 (0.5) 4–5 3 4.7 (0.6) 4–5 Became part of our primary care team 9 4.1 (0.6) 3–5 6 3.8 (1.0) 3–5 Benefited my patients 9 4.8 (0.4) 4–5 2 5.0 (0.0) 5 Helped my patients receive treatment more quickly 9 4.8 (0.4) 4–5 6 5.0 (0.0) 5 I would recommend this service to other colleagues 9 4.4 (0.7) 3–5 6 4.1 (1.0) 3–5 I would like the integrated behavioral health service to continue 9 4.7 (0.5) 4–5 6 4.7 (0.5) 4–5 Note. The ns vary because some providers chose “Not Applicable” for a response. 135INTEGRATING BEHAVIORAL HEALTH SERVICES
- 110. na l u se o f t he in di vi du al u se r a nd is n ot to b e di ss em
- 111. in at ed b ro ad ly . tients benefited from seeing the BHPs. Both PCPs and nurses would recommend this service to other colleagues within college health and would like IBHC to continue in the future. Patient Satisfaction Results of the satisfaction assessment indi- cate that a majority of the sample of patients were satisfied with their overall care at SUHS (see Table 3). A number of students did not remember filling out the screening question- naire (n � 13, 17%) or meeting with a BHP (n � 26, 33%), so they did not rate their satis- faction or report on those elements of the IBHC program in Table 3. Of those who remembered completing the questionnaire, the majority re- ported that they talked to the medical provider about a topic on the screening measure (n � 57, 86%). Of those who remembered meeting with a BHP, the majority reported that they felt that the BHP helped them with the topic that they
- 112. discussed (n � 38, 73%). As shown in Table 3, overall participants reported a general level of comfort filling out the screening measure, were satisfied with the service provided by the integrated BHP, and would be willing to seek help from the BHP again if necessary. Although the average re- sponse was within a level of agreement (M � 3.6), there was a greater level of variabil- ity when it came to having the service within the university health setting as compared with a specialty mental health clinic on campus, with a mode of 3.0 indicating a neutral response. Discussion As expected, this study found that PCPs, nurses, and patients reported positive experi- ences with the two major components of the IBHC program: the implementation of a behav- ioral health screening assessment and the inte- gration of BHPs into the university health cen- ter. The results provide further evidence that this model of care can be used on college cam- puses with success in terms of provider and patient satisfaction. Similar to past research (Alschuler et al., 2008; Cowan & Morewitz, 1995), this study found that providers indicated that having brief screening items to assess sleep problems, de- pression, alcohol use, and tobacco use was help- ful to their clinical practice. In addition, the assessment items reportedly helped stimulate
- 113. discussions with patients about topics that would not have otherwise been discussed. Alschuler and colleagues (2008) found a similar result such that those providers whose patients Table 3 Patient Ratings of IBHC Satisfaction and Acceptability Item n Mode M SD Range Rate your overall level of satisfaction with the visit(s) you had at University Health Service 79 4.0 3.4 1.1 1–5 Rate your level of comfort filling out the screening questionnaire during your visit 66 4.0 3.5 1.1 1–5 Rate your level of satisfaction with the service you were provided during the visits with the integrated behavioral health provider 52 4.0 3.4 1.2 1–5 Rate your level of willingness meet with one of those providers again if something else or that issue continued 52 4.0 3.4 1.4 1–5 Rate your level of comfort meeting with them at University Health Service rather than some other location on campus (e.g., SU Counseling Center) 52 3.0 3.6 1.0 2–5 Rate your level of comfort with the length of the meetings (i.e., typically less than 40 minutes) with the integrated behavioral health provider 52 4.0 3.7 0.9 2–5
- 114. 136 FUNDERBURK, FIELDER, DEMARTINI, AND FLYNN T hi s do cu m en t i s co py ri gh te d by th e A m er ic an
- 117. so na l u se o f t he in di vi du al u se r a nd is n ot to b e di ss
- 118. em in at ed b ro ad ly . were randomly assigned to fill out a mental health questionnaire discussed those issues with their patients more than those providers whose patients were not assigned to fill out the ques- tionnaire. Not only did providers perceive the screening questionnaire as having a high level of utility within their clinical practice, but the patients also reportedly were comfortable with filling out the questionnaire during their ap- pointments. Our findings highlight the importance of se- lecting an appropriate screening questionnaire that can be completed and scored quickly. A common concern among providers when dis- cussing the implementation of regular screening for mental health issues is the time involved in integrating the screen within the clinical ap- pointment (Thomas, Waxmonsky, McGinnis, & Barry, 2006). Within this study, a majority of
- 119. the providers and nurses reported responses within the neutral range when asked about whether the screening measure took time away from other clinical duties. This is not surprising as the questionnaire obviously does add time to the patient visit, as noted in prior research (Alschuler et al., 2008). The typical patient ap- pointment at this clinic is only 15 minutes, so allocating 1–2 minutes to review the screen with the patient would reduce the time left to focus on the patient’s presenting complaint. The fact that providers endorsed a modal response within the neutral range suggests that the screening can be incorporated without a signif- icant negative impact. One study on behavioral health screening found that using a measure that includes areas specific to college students (e.g., academic stress, risky sexual behavior) im- proved detection of students struggling with adjustment issues compared to a more general screening measure (Alschuler, Hoodin, & Byrd, 2009). However, the benefit of added sensitivity from a college-specific screening measure may not offset the cost of greater administration and scoring time. As completion time increases, the rate of compliance with screening may de- crease. Another element that was identified within this study was the importance of not only de- signing the screening questionnaire to be easily comprehended by patients but to make sure it is easily scored and interpreted by providers. Most providers did not indicate difficulty scoring or interpreting the screen. However, anecdotally
- 120. there were some problems with patients incor- rectly self-scoring the PHQ-9; this may have led to some confusion or the need for providers to double-check or recalculate scores. The screen- ing tool was later modified to discourage pa- tients from totaling their own scores. To maxi- mize screening coverage and efficiency, it is important to select brief, user-friendly, vali- dated measures that are easy to score and inter- pret (Kirkcaldy & Tynes, 2006). As university health centers work toward im- proving the identification and treatment of men- tal health issues as well as implementing rec- ommended screening guidelines for depression, suicidal ideation, tobacco use, and alcohol mis- use, this study suggests that an IBHC program may be one way to effectively accomplish this while maintaining provider and patient satisfac- tion. A previous study of behavioral health screening in university health centers found that screening increased discussion of behavioral health issues among patients and PCPs (Alschuler et al., 2008). However, PCPs re- ported that they did not have the time or the expertise to adequately address behavioral health issues with patients, but they were open to collaborating with BHPs. Likewise, our re- sults suggest high willingness to refer patients to BHPs to improve attention to behavioral health issues. Thus, the IBHC program can help PCPs deal with positive screens by providing the integrated BHPs, who are trained to assess mental health issues and provide brief treatment on-site or facilitate a referral to a specialty men- tal health clinic.
- 121. Regarding the integrated BHPs component of the IBHC program, PCPs also strongly indi- cated that their patients benefited from the ser- vices provided by the BHPs. The providers felt that having the integrated BHPs helped patients receive treatment faster (compared to referring them to specialty mental health) and that the BHPs functioned as part of the overall care team. All of the providers reported that they would strongly recommend the IBHC to other colleagues working in college health. Taken together, these results indicate satisfaction among the medical providers, which is essential for the success of IBHC. Strong buy-in on the part of PCPs is needed to sustain the implemen- tation of a new clinical program like IBHC, which requires procedural changes and addi- tional effort (i.e., reviewing screens, referring 137INTEGRATING BEHAVIORAL HEALTH SERVICES T hi s do cu m en t i s co
- 124. in te nd ed s ol el y fo r t he p er so na l u se o f t he in di vi du
- 126. patients to BHPs). Acceptability among the nurses is also important, as they were the ones responsible for offering patients the behavioral health screens in our IBHC program. Similarly, satisfaction and acceptability were high among patients. Patients who were seen by BHPs reported feeling comfortable with the ser- vices received and were willing to be seen again should the service be needed in the future. These results corroborate Westheimer and Steinley-Bumgarner’s (2008) finding that pa- tients were accepting of referrals to BHPs. Pa- tients may like the convenience of being seen quickly by BHPs in health centers. In the case of BHPs having open access schedules, patients can be seen immediately after their PCP visit, which eliminates the need for scheduling an- other appointment or returning to the health center; in contrast, specialty mental health cen- ters may have long (e.g., up to 2–3 weeks) wait times (Mowbray et al., 2006). Also, health cen- ters carry less stigma compared with specialty mental health settings. On average, the patients were comfortable seeking services at the uni- versity health center, but there was a greater level of variability suggesting some individual differences as to the comfort of seeking those services at a specialty mental health clinic. Limitations Interpretation of the findings should take into account the limitations of the study. First, al- though slightly higher than that found in other research using similar methodology (Shih &
- 127. Fan, 2009), our response rate for the patient satisfaction survey was 29%. The response rate may be improved by contacting patients soon after their final IBHC visit instead of at the end of each semester, which is generally a busy time for students. Second, a significant proportion of the patients did not remember completing the screening questionnaire or meeting with a BHP. Patients may not have remembered completing the screening questionnaire because it was a brief (i.e., 2–3 minutes) activity and/or because their health center visit was up to four months before completing the satisfaction survey. It is possible that the students who did not remember meeting with a BHP had a more neutral expe- rience than the students who remembered the program. Thus, the satisfaction ratings could be artificially elevated because of this lack of data. It is also possible, however, that these students did not remember the meeting with the BHP because they simply considered the components of the IBHC part of standard medical care. Authors have noted that primary care has be- come the “de facto mental health care system” (Kessler & Stafford, 2008, p. 9), so these stu- dents may have expected to discuss behavioral health problems during their visit and may not have perceived the BHP as different from a regular medical provider. Third, patient data were obtained via anony- mous self-report. Though this method of data collection was necessary because of the scope of this study, it prohibited collection of identi- fying information, including diagnostic infor-
- 128. mation. The ability to compare satisfaction across diagnostic categories would have pro- vided beneficial information, including whether patients with more severe diagnoses (e.g., major depressive disorder vs. adjustment disorder with depressed mood) had equally positive experi- ences with the program. In addition, the satis- faction ratings are limited to only those patients who were seen by an integrated BHP. Future research should compare satisfaction between patients seen within IBHC and patients seen within standard care (i.e., the PCP provides any treatment for behavioral health concerns or makes a referral to specialty mental health). Fourth, the provider and patient satisfaction measures were created specifically for this study. The limited range of response options (1–5) may contribute to restricted range/ variability and ceiling effects. These limitations should not be ignored when considering the generalizability of the study. Finally, the scope of this study did not allow us to obtain information on the clinical out- comes associated with the IBHC program. Al- though providers reported that patients benefit- ted from meeting with BHPs, their perceptions were based solely on behavioral observations of and/or self-report from patients, not on clinical outcome data. Future research should evaluate the clinical effectiveness of interventions deliv- ered by integrated BHPs. From an IBHC per- spective, other markers of success that are wor- thy of future study include increased access to mental/behavioral health services, improved identification of mental/behavioral health issues
- 129. through screening, increased referral uptake (i.e., BHPs referral attendance compared to spe- 138 FUNDERBURK, FIELDER, DEMARTINI, AND FLYNN T hi s do cu m en t i s co py ri gh te d by th e A m er
- 132. p er so na l u se o f t he in di vi du al u se r a nd is n ot to b e
- 133. di ss em in at ed b ro ad ly . cialty mental health referral attendance) attrib- utable to colocation and “warm hand-offs,” im- proved provider communication (e.g., between BHPs and PCPs), reduced burden on specialty mental health centers from patients with sub- threshold or mild symptoms, and reduced bur- den on PCPs from repeat visits because of psy- chosocial issues. Conclusions In summary, providers and patients indicated a high level of satisfaction with this IBHC pro- gram. Accordingly, providers are likely to refer patients to BHPs, and patients are likely to engage in brief treatment within the IBHC pro- gram. Given the increasing demand on univer-
- 134. sity primary care clinics to address the mental health needs of students, IBHC offers a prom- ising method whereby to address this need. Par- ticularly in light of data that indicate that most college students do not seek needed mental health treatment (Rosenthal & Wilson, 2008), the finding that IBHC patients would feel com- fortable seeing a BHP again in the future is a positive step toward making mental health care more accessible to patients who need treatment. References Alschuler, K., Hoodin, F., & Byrd, M. (2008). The need for integrating behavioral care in a college health center. Health Psychology, 27, 388 –393. doi:10.1037/0278-6133.27.3.388 Alschuler, K. N., Hoodin, F., & Byrd, M. R. (2009). Rapid assessment for psychopathology in a college health clinic: Utility of college student specific questions. Journal of American College Health, 58, 177–179. doi:10.1080/ 07448480903221210 American Academy of Pediatrics. (2001). Alcohol use and abuse: A pediatric concern. Pediatrics, 108, 185–189. doi:10.1542/peds.108.1.185 American College Health Association. (2010a). American College Health Association National College Health Assessment II: Reference Group Executive Summary Spring 2010. Linthicum, MD: Author. American College Health Association. (2010b). Con-
- 135. siderations for integration of counseling and health services on college and university cam- puses. Journal of American College Health, 58, 583–596. doi:10.1080/07448481.2010.482436 Bastien, C. H., Valliéres, A., & Morin, C. M. (2002). Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Medicine, 2, 297–307. doi:10.1016/S1389- 9457(00)00065-4 Blount, A., Schoenbaum, M., Kathol, R., Rollman, B. L., Thomas, M., O’Donohue, W., & Peek, C. J. (2007). The economics of behavioral health ser- vices in medical settings: A summary of the evi- dence. Professional Psychology: Research and Practice, 38, 290 –297. doi:10.1037/0735- 7028.38.3.290 Bryan, C. J., Morrow, C., & Appolonio, K. K. (2009). Impact of behavioral health consultant interven- tions on patient symptoms and functioning in an integrated family medicine clinic. Journal of Clinical Psychology, 65, 281–293. doi:10.1002/ jclp.20539 Christmas, W. A. (1995). The evolution of medical services for students at colleges and universities in the United States. Journal of American College Health, 43, 241–246. doi:10.1080/07448481 .1995.9940897 Cigrang, J. A., Dobmeyer, A. C., Becknell, M. E., Roa-Navarrete, R. A., & Yerian, S. R. (2006). Evaluation of a collaborative mental health pro-
- 136. gram in primary care: Effects on patient distress and health care utilization. Primary Care & Com- munity Psychiatry, 11, 121–127. doi:10.1185/ 135525706X121192 Cowan, P. F., & Morewitz, S. J. (1995). Encouraging discussion of psychosocial issues at student health visits. Journal of American College Health, 43, 197–200. doi:10.1080/07448481.1995.9940476 Eisenberg, D., Golberstein, E., & Gollust, S. E. (2007). Help-seeking and access to mental health care in a university student population. Medical Care, 45, 594 – 601. doi:10.1097/ MLR.0b013e31803bb4c1 Fitzpatrick, R. (1991). Surveys of patient satisfac- tion: I—Important general considerations. British Medical Journal, 302, 887– 889. doi:10.1136/ bmj.302.6781.887 Gallo, J. J., Zubritsky, C., Maxwell, J., Nazar, M., Bogner, H. R., Quijano, L. M., . . . Levkoff, S. E., & the PRISM-E investigators (2004). Primary care clinicians evaluate integrated and referral models of behavioral health care for older adults: Results from a multisite effectiveness trial (PRISM-E). Annals of Family Medicine, 2, 305– 309. doi:10.1370/afm.116 Garlow, S. J., Rosenberg, J., Moore, J. D., Haas, A. P., Koestner, B., Hendin, H., & Nemeroff, C. B. (2008). Depression, desperation, and sui- cidal ideation in college students: Results from the American Foundation for Suicide Prevention College Screening Project at Emory University.
- 137. Depression and Anxiety, 25, 482– 488. doi: 10.1002/da.20321 Goodie, J. L., Isler, W. C., Hunter, C., & Peterson, 139INTEGRATING BEHAVIORAL HEALTH SERVICES T hi s do cu m en t i s co py ri gh te d by th e A m
- 140. he p er so na l u se o f t he in di vi du al u se r a nd is n ot to b
- 141. e di ss em in at ed b ro ad ly . A. L. (2009). Using behavioral health consultants to treat insomnia in primary care: A clinical case series. Journal of Clinical Psychology, 65, 294 – 304. doi:10.1002/jclp.20548 Kessler, R., & Stafford, D. (2008). Primary care is the de facto mental health system. In R. Kessler & D. Stafford (Eds.), Collaborative medicine case studies: Evidence in practice (pp. 9 –21). New York: Springer. doi:10.1007/978-0-387-76894- 6_2 Kirkcaldy, R. D., & Tynes, L. L. (2006). Depression screening in a VA primary care clinic. Psychiatric Services, 57, 1694 –1696. doi:10.1176/appi.ps
- 142. .57.12.1694 Masters, K. M., Stillman, A. M., Browning, A. D., & Davis, J. W. (2005). Primary care psychology training on campus: Collaboration within a stu- dent health center. Professional Psychology: Re- search and Practice, 36, 144 –150. doi:10.1037/ 0735-7028.36.2.144 Mills, D., Gold, R., & Curran, M. (1996). Healthcare reform: A survey of college health services. Jour- nal of American College Health, 45, 106 –117. doi:10.1080/07448481.1996.9936870 Mowbray, C. T., Megivern, D., Mandiberg, J. M., Strauss, S., Stein, C. H., Collins, K., . . . Lett, R. (2006). Campus mental health services: Recom- mendations for change. American Journal of Or- thopsychiatry, 76, 226 –237. doi:10.1037/0002- 9432.76.2.226 Nimalasuriya, K., Compton, M. T., Guillory, V. J., & Prevention Practice Committee of the American College of Preventive Medicine. (2009). Screen- ing adults for depression in primary care: A po- sition statement of the American College of Pre- ventive Medicine. Journal of Family Practice, 58, 535–538. Reiss-Brennan, B., Briot, P., Daumit, G., & Ford, D. (2006). Evaluation of “depression in primary care” innovations. Administration and Policy in Mental Health and Mental Health Services Re- search, 33, 86 –91. doi:10.1007/s10488-005- 4239-x
- 143. Rosenthal, B., & Wilson, W. C. (2008). Mental health services: Use and disparity among diverse college students. Journal of American College Health, 57, 61– 68. doi:10.3200/JACH.57.1.61-68 Runyan, C. N., Fonseca, V. P., & Hunter, C. (2003). Integrating consultive behavioral healthcare into the Air Force Medical System. In W. T. O’Donohue, K. E. Ferguson, & N. A. Cummings (Eds.), Behavioral health as primary care: Be- yond efficacy to effectiveness (pp. 145–163). Reno, NV: Context Press. Saunders, J. B., Aasland, O. G., Babor, T. F., de la Fuente, J. R., & Grant, M. (1993). Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol con- sumption, II. Addiction, 88, 791– 804. doi: 10.1111/j.1360-0443.1993.tb02093.x Shih, T., & Fan, X. (2009). Comparing response rates in e-mail and paper surveys: A meta-analysis. Educational Research Review, 4, 26 – 40. doi: 10.1016/j.edurev.2008.01.003 Sitzia, J., & Wood, N. (1997). Patient satisfaction: A review of issues and concepts. Social Science & Medicine, 45, 1829 –1843. doi:10.1016/S0277- 9536(97)00128-7 Spitzer, R. L., Kroenke, K., & Williams, J. B. W. (1999). Validation and utility of a self-report ver- sion of PRIME-MD: The PHQ primary care study. JAMA: Journal of the American Medical