CONTENTS
◦ Introduction
◦ Evolutionof concept of loading
◦ Classification of loading protocols
◦ Osseointegration
◦ Progressive loading protocol
◦ Elements of progressive loading
◦ Immediate loading
◦ Rationale of immediate loading
◦ Guidelines of immediate loading
◦ Density of bone – type of loading
◦ Approaches to reduce loading period
◦ Conclusion
◦ References
3.
INTRODUCTION
◦ In thelast two decades, dental implants have become a reliable way to replace
missing teeth.
◦ Earlier, the Branemark two-stage method was used, where implants were placed
under the gingiva and left to heal for 3–6 months before adding the prosthesis.
◦ This method was developed by Branemark after many years of research, and the
implants were expected to last for many years.
◦ Later studies showed that implants could sometimes be loaded earlier, using a
one-stage approach.
4.
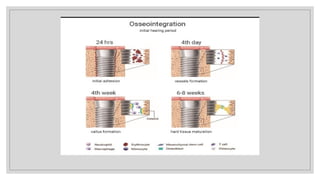
OSSEOINTEGRATION
There are twobasic theories regarding the bone implant interface.
1) Fibro-osseous integration-supported by Linkow (1970), James (1975), and Weiss
(1986).
2) Osseointegration supported by Branemark (1985).
A direct and stable contact between living bone and the implant surface without
any soft tissue in between them.
6.
DENSITY OF BONE-TYPE OF LOADING
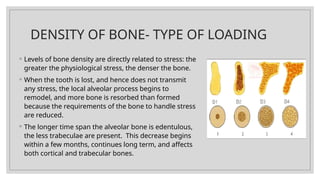
◦ Levels of bone density are directly related to stress: the
greater the physiological stress, the denser the bone.
◦ When the tooth is lost, and hence does not transmit
any stress, the local alveolar process begins to
remodel, and more bone is resorbed than formed
because the requirements of the bone to handle stress
are reduced.
◦ The longer time span the alveolar bone is edentulous,
the less trabeculae are present. This decrease begins
within a few months, continues long term, and affects
both cortical and trabecular bones.
7.
BONE IMPLANT INTERFACE
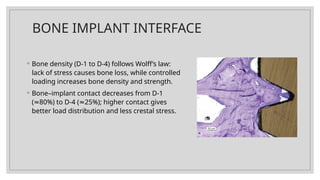
◦Bone density (D-1 to D-4) follows Wolff’s law:
lack of stress causes bone loss, while controlled
loading increases bone density and strength.
◦ Bone–implant contact decreases from D-1
( 80%) to D-4 ( 25%); higher contact gives
≈ ≈
better load distribution and less crestal stress.
8.
◦ Lamellar boneis ideal for implant support but takes up to 1 year to fully
mineralize; early healing bone is mainly woven bone and weak.
◦ Healing time increases as bone density decreases: D-1: 5 months, D-2: 4 months,
D-3: 6 months, D-4: 8 months before second-stage surgery.
◦ Successful osseointegration depends on bone quality, bone contact, healing
time, and gradual functional loading to prevent overload and bone resorption.
9.
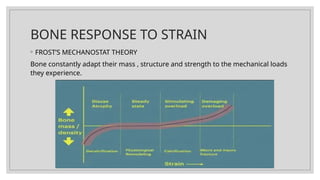
BONE RESPONSE TOSTRAIN
◦ FROST’S MECHANOSTAT THEORY
Bone constantly adapt their mass , structure and strength to the mechanical loads
they experience.
10.
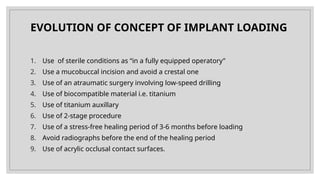
EVOLUTION OF CONCEPTOF IMPLANT LOADING
1. Use of sterile conditions as “in a fully equipped operatory”
2. Use a mucobuccal incision and avoid a crestal one
3. Use of an atraumatic surgery involving low-speed drilling
4. Use of biocompatible material i.e. titanium
5. Use of titanium auxillary
6. Use of 2-stage procedure
7. Use of a stress-free healing period of 3-6 months before loading
8. Avoid radiographs before the end of the healing period
9. Use of acrylic occlusal contact surfaces.
11.
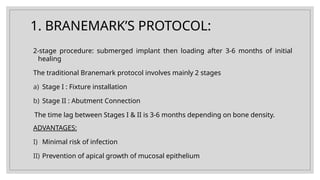
1. BRANEMARK’S PROTOCOL:
2-stageprocedure: submerged implant then loading after 3-6 months of initial
healing
The traditional Branemark protocol involves mainly 2 stages
a) Stage I : Fixture installation
b) Stage II : Abutment Connection
The time lag between Stages I & II is 3-6 months depending on bone density.
ADVANTAGES:
I) Minimal risk of infection
II) Prevention of apical growth of mucosal epithelium
12.
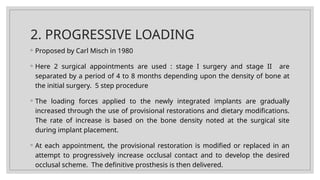
2. PROGRESSIVE LOADING
◦Proposed by Carl Misch in 1980
◦ Here 2 surgical appointments are used : stage I surgery and stage II are
separated by a period of 4 to 8 months depending upon the density of bone at
the initial surgery. 5 step procedure
◦ The loading forces applied to the newly integrated implants are gradually
increased through the use of provisional restorations and dietary modifications.
The rate of increase is based on the bone density noted at the surgical site
during implant placement.
◦ At each appointment, the provisional restoration is modified or replaced in an
attempt to progressively increase occlusal contact and to develop the desired
occlusal scheme. The definitive prosthesis is then delivered.
13.
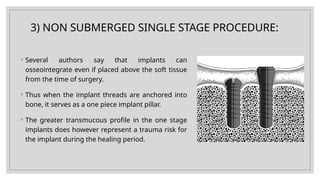
3) NON SUBMERGEDSINGLE STAGE PROCEDURE:
◦ Several authors say that implants can
osseointegrate even if placed above the soft tissue
from the time of surgery.
◦ Thus when the implant threads are anchored into
bone, it serves as a one piece implant pillar.
◦ The greater transmucous profile in the one stage
implants does however represent a trauma risk for
the implant during the healing period.
14.
ADVANTAGES
1. One stagesurgical procedure - Less chair time, Less pain, Shorter healing
period
2. No microgap at alveolar crest bone level - Less crestal bone resorption,
during healing and following initiation of functional loading
3. Implant shoulder at soft tissue level so Implant easily accessible for
prosthetic procedures
15.
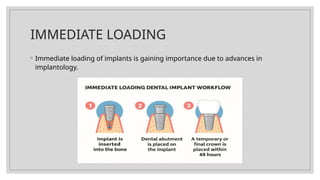
4. IMMEDIATE FUNCTIONALLOADING
◦ This technique of placing Implants in a single surgical step involves fitting the
prosthesis in the same surgical session.
◦ According to some it may be delayed by up to 3 days post surgery.
◦ The Provisional restoration delivered is in full occlusal contact with the opposing
dentition.
◦ The advantage of this method in addition to the surgery taking place in single
step, is the immediate fitting of the final prosthesis and the patient’s failure to
experience any functional & psychological discomfort associated with being
edentulous.
16.
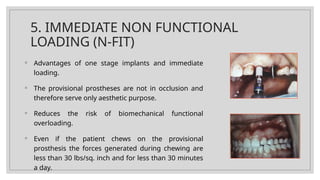
5. IMMEDIATE NONFUNCTIONAL
LOADING (N-FIT)
◦ Advantages of one stage implants and immediate
loading.
◦ The provisional prostheses are not in occlusion and
therefore serve only aesthetic purpose.
◦ Reduces the risk of biomechanical functional
overloading.
◦ Even if the patient chews on the provisional
prosthesis the forces generated during chewing are
less than 30 lbs/sq. inch and for less than 30 minutes
a day.
17.
6. EARLY LOADING
◦The final prosthesis is fitted 3 weeks after surgery .
◦ Some regard it as delivery of a prosthetic implant suprastructure from 3 days
up to 6 weeks post surgery.
18.
7. DELAYED LOADING
Accordingto some authors, implants subjected to loading after more than 6 weeks
post surgery are said to come under delayed loading, as per the standard
protocol.
8. ANTICIPATED LOADING
Here, provisional prosthesis is fitted about 2 months after the surgery.
19.
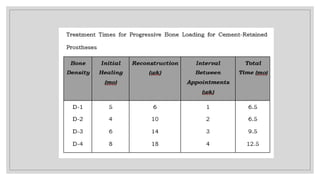
PROGRESSIVE BONE LOADING
◦By Misch in 1980.
◦ Implant stability was evaluated over two years using the Periotest, which
measures implant mobility and damping.
◦ Implants initially showed positive Periotest values, which became negative over
time, indicating increased stability after functional loading.
◦ Although the relationship between load, time, and bone density is not linear, a
safe clinical protocol was developed.
◦ The protocol includes two surgical stages and five prosthodontic steps, with time
intervals and gradual load increase based on bone density.
20.
◦ D-1 bonehas high initial bone contact and lamellar bone; prosthodontic visits
can be 1 week apart, and progressive loading is least critical.
◦ D-2 bone responds well to functional loads; prosthetic appointments are spaced
2 weeks apart, with total treatment time about 6½ months.
◦ D-3 bone has less cortical bone and fine trabeculae; appointments are spaced 3
weeks apart, and treatment takes about 10 months, allowing bone quality and
mineralization to improve.
◦ Progressive loading becomes increasingly important in D-3 bone due to lower
initial bone contact.
◦ D-4 bone requires the most cautious approach, with appointments 4 weeks or
more apart and a total treatment time of at least 12½ months to allow mature
bone formation.
22.
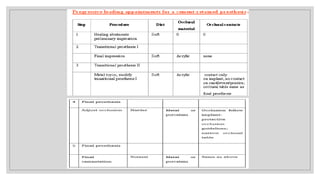
Elements of progressiveloading
◦ Time interval
◦ Diet
◦ Occlusal material
◦ Occlusal contacts
◦ Prosthesis design
23.
TIME
◦ initial implantplacement and Stage II uncovery - 3 to 8 months
◦ D1 & D2 - 3 to 4 months
◦ D3 &D4 - 5 to 6 months
◦ Immature bone – 8 months
24.
DIET
1. Control diet–prevent overloading at early phase.
2. The initial healing phase- avoid chewing in the area.
3. Uncovered,implant connected to a high abutment - greater risk - soft diet( 10
psi).
4. After initial delivery of the final prosthesis –meat (21psi)
5. After final evaluation – raw vegetables (27psi)
25.
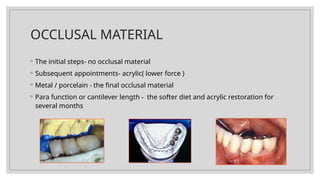
OCCLUSAL MATERIAL
◦ Theinitial steps- no occlusal material
◦ Subsequent appointments- acrylic( lower force )
◦ Metal / porcelain - the final occlusal material
◦ Para function or cantilever length - the softer diet and acrylic restoration for
several months
26.
OCCLUSION
◦ Gradually intensifiesthe occlusal contacts during initial healing.
◦ First transitional prosthesis - out of occlusion.
◦ Final restoration implant-protective occlusion.
PROSTHESIS DESIGN
◦ Transitional acrylic restoration - no occlusal contact and no cantilevers.
◦ The second acrylic transitional restoration- occlusal contact similar to final
restorations and no cantilevers except in the esthetics zone.
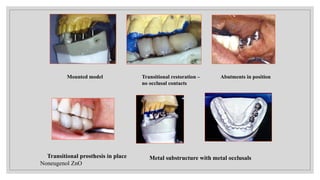
29.
Mounted model Transitionalrestoration –
no occlusal contacts
Abutments in position
Transitional prosthesis in place
Noneugenol ZnO
Metal substructure with metal occlusals
30.
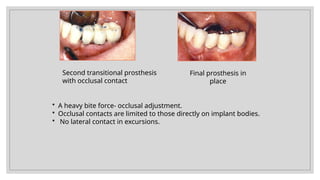
Second transitional prosthesis
withocclusal contact
Final prosthesis in
place
• A heavy bite force- occlusal adjustment.
• Occlusal contacts are limited to those directly on implant bodies.
• No lateral contact in excursions.
◦ INDICATIONS:
◦ Singletooth replacement
◦ Partial edentulism
◦ Full edentulism.
◦ CONTRAINDICATIONS:
◦ Patients who are bruxers.
◦ Edentulous patients with a reduced bone quality and quantity.
◦ With not optimized biomechanically suprastructures.
◦ With short implant lengths.
33.
ADVANTAGES
1) Immediate fullfunction of the new tooth.
2) It gives beautiful, natural cosmetic appearance.
3) Very little discomfort is associated with the procedure. In fact some people have
reported almost no pain at all.
4) This procedure is less invasive than some older procedures for crown and bridge
placement, where perfectly good neighboring teeth have to be ground down to
accommodate the crown.
5) Long term edentulism can be eliminated.
6) No additional appointments are required
34.
DISADVANTAGES
1) More chancesof failure.
2) Peri-implant bone reaction is highest after surgical trauma due to immediate
loading.
3) High chances of post-operative complications.
4) More patient co-operation is needed.
5) More bone loss compared to delayed loading.
35.
STEPS
1. Pre-surgical planning
◦Case selection based on bone quality, quantity, and occlusion
◦ Provisional fixed restoration is fabricated before surgery
◦ Prefer edentulous arches (mandibular interforaminal region)
2. Surgical implant placement
◦ Implants placed using a meticulous, minimally traumatic technique with copious irrigation
◦ Bone quality and primary stability assessed during osteotomy
◦ Use threaded, rough-surface implants ( 10 mm length), optimal diameter, and bicortical
≥
engagement when possible
◦ Avoid tapping to preserve bone
36.
3. Assessment ofprimary stability
◦ Immediate loading proceeds only if adequate primary stability is achieved
◦ Dense bone (D-1, D-2, or good D-3) preferred
4.Abutment and prosthetic cylinder connection
◦ Abutments and prosthetic cylinders connected immediately after implant placement
◦ Ensures correct implant position relative to the prosthesis
5. Conversion of provisional prosthesis
◦ Pre-fabricated provisional is converted into a fixed, non-removable implant-supported
prosthesis
◦ Prosthetic cylinders are picked up intraorally using autopolymerizing acrylic resin
◦ Conversion completed before flap closure for precise fit
37.
6. Immediate prosthesisdelivery
◦ Screw-retained provisional restoration preferred
◦ Restoration should not be removed during healing to prevent micromotion
◦ Provides splinting effect and cross-arch stabilization
7. Occlusal adjustment
◦ Light, controlled occlusion with reduced cusp inclines
◦ Lingualized occlusion, narrow opposing cusps, shallow fossae
◦ Cantilevers avoided
8. Healing and functional evaluation
◦ Patient wears the provisional during osseointegration
◦ Esthetics, phonetics, and function evaluated over healing period
◦ Healing time: ~3 months (mandible), 5–6 months (maxilla)
38.
9. Final impressionand definitive prosthesis
◦ Impressions taken at surgery or later using the acrylic splinted provisional
◦ Final restoration fabricated after confirmed osseointegration
10. Post-operative care
◦ Soft diet advised
◦ Caution in bruxers and smokers
◦ Progressive functional loading supports bone maturation and long-term implant success
39.
APPROACHES TO REDUCELOADING
PERIOD
Three different approaches are relevant :
1. To optimize the healing period before a safe functional loading can be exerted
on free standing implants. This should be achieved by reducing stepwise the
delayed loading periods, below the traditional 3-6 months.
2. To identify, upon immediate loading, an effective way to reduce micro – motion
beneath the critical threshold of deleterious micro-motion.
3. Careful patient selection
40.
1) Optimization OfThe Healing Period
For Free-Standing Implants:
◦ Based on Brånemark , it is suggested that healing periods shorter than 3 months in the
mandible may still be predictable. shorter healing periods should be limited to Type I and
Type II bone, as implant success is strongly influenced by recipient site quality.
◦ Implant surface characteristics also play an important role in early loading.
◦ Rough-surface implants, such as those treated with titanium plasma spraying, may allow
earlier loading compared to smooth-surface implants.
◦ These surfaces demonstrate faster bone apposition, greater bone-implant contact, and
stronger fixation during healing, as shown by torque measurements.
41.
2) Reducing Micro-MotionBeneath The
Threshold Of Deleterious Micro-Motion:
◦ For implant-retained overdentures
1) Splinting of 3-4 implants in the interforaminal area aimed to reduce the amount
of micromotion was successful up to certain extent. The success rates reported in
the literature for implant-retained overdentures with implants healed in the
traditional way
2) Bicortical anchorage in adequate bone quality
3) Implant length
42.
◦ For implantretained fixed restoration
1. Developed by Schnitman et al (1990), it involves insertion in the anterior and
posterior regions of “primary and secondary implants”. The latter sustains a
provisional prosthesis in broad-based tripod configuration and permit the “
primary “ implants to be incorporated in a definitive restoration.
2. It involves a higher number of implants, 6 to 10 implants, all immediately
loaded in the provisional restoration.
43.
EARLY LOADING PROTOCOLS:
◦Need for re-evaluation of Branemark protocol :
◦ The following 4 reasons may provide cause to reevaluate the mandatory aspect
of a long delayed loading period. They are :
1. Consideration to be given to the specifically demanding conditions met during
the original Branemark follow-up
2. Loading per se does not impede the healing process to occur,
3. Prematurely loaded implants are capable of integration as demonstrated in
several experimental studies.
4. Prematurely loaded implants are capable of clinical integration as observed by
various authors.
44.
CONCLUSION
◦ Implants restorefunction, esthetics, bone and soft tissue contours, speech and
intra oral health.
◦ Delayed healing process may cause psychological, social , speech and function
problems.
◦ Immediate restoration after implant surgery is one of the alternatives.
◦ Careful patient screening and selection required.
45.
REFERENCES
Misch C.E.Contemporary implant dentistry. Mosby Publishing Company.
Babush C. Dental implants- Principles and Practice" W.B. Saunder's Company.
Schnitman PA, Wohrle PS, Rubenstein JE. Ten years results for Branemark
implants immediately loaded with fixed prostheses at implant placement. Int J
Oral Maxillofac Implants 1997;12(4):495-503.
Tarnow DP, Emtiaz S, Classi A. Immediate Loading of threaded implants at stage
1 surgery in edentulous arches: ten consecutive case reports with 1 to 5 year
data. Int J Oral Maxillofac Implants 1997:12(3):319-24.
Editor's Notes
#10 The predictability of implant integration according to Branemark and collaborators was obtained by adherence to a strict surgical and prosthodontic protocol.
#41 Another way to shorten the delayed loading period is to find an effective prosthetic option that maintains the amount of micro-motion beneath the threshold of deleterious micromotion during the healing phase.
















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
