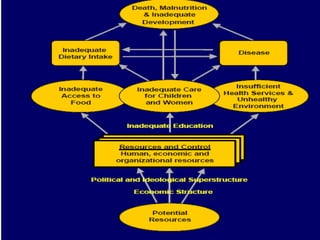
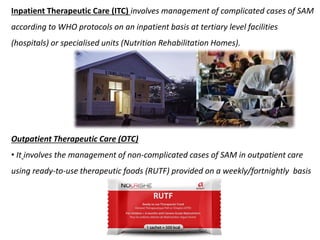
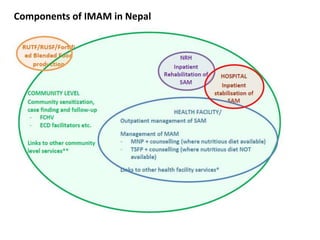
The document provides an overview of Integrated Management of Acute Malnutrition (IMAM) in Nepal. IMAM aims to reduce mortality and morbidity from acute malnutrition through four components: community mobilization to identify cases, inpatient care for complicated cases, outpatient care using ready-to-use therapeutic foods for non-complicated cases, and management of moderate acute malnutrition through supplementary feeding or micronutrient powders. The principles of IMAM are to achieve maximum coverage and access through community-based services, prioritize timely treatment, and provide appropriate care until recovery.



























































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)







![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)



