Lecture 8 - Technology, Innovation and Great Power Competition - Cyber
IGI Technologies I-Corps@NIH 121014
1. Team 10 - Team IGI Tech
Lessons Learned
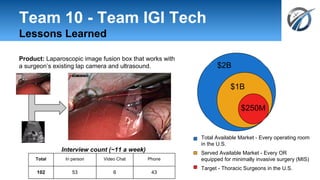
Product: Laparoscopic image fusion box that works with
a surgeon’s existing lap camera and ultrasound.
Interview count (~11 a week)
Total In person Video Chat Phone
102 53 6 43
$2B
$1B
$250M
Total Available Market - Every operating room
in the U.S.
Served Available Market - Every OR
equipped for minimally invasive surgery (MIS)
Target - Thoracic Surgeons in the U.S.
2. IGI Technologies Team
Principal Investigator
Raj
Shekhar, PhD
Industry Expert
Mark
Chandler, MBA
Entrepreneur
William
Plishker, PhD
● Principal investigator within the
Sheikh Zayed Institute for
Pediatric Surgical Innovation
● Focuses on clinically driven
innovation
● 15 years of experience as a
serial innovator of medical and
surgical imaging technologies
● Two of his prior inventions have
led to commercial products.
● CEO of IGI Technologies
● Builder and leader of
startups, converting
academic research into
real-world products.
● 3 Different Silicon Valley
startups as an engineer
and marketer
● Mayfield Fellow
● Early stage medical
device investor
● Expert in commercializing
intellectual property (IP)
● Founder of Upstream
Partners
● CEO of TAO Lifesciences
5. So here’s what we did:
Experiment: Talk to a wide variety of lap
surgeons outside of home institution
Insight: Very first interview, many lap surgeons
do not have ultrasound, and do not want it.
6. We talked to surgeons - and learned we didn’t
know them as well as we thought
Surgeon Value Propositions Surgeon Pains/Gains
Products/
services
Overlay
ultrasound
on lap field
of view
Guidance
of ablative
tools
Gain creators
Get to target more reliably
than standalone ultrasound
Get to target faster than
standalone ultrasound
Find targets
Pain relievers
Single display
Lower technical difficulty
Reduce risk of complication
Customer Job(s)
Lap surgery --
ablation/resection
Pre-procedure --
diagnose
Post procedure patient
monitoring
Often no task for
ultrasound
Gains
Belief in better patient care
More confidence in complete
treatment
More lap target identification,
less open surgeon
Faster procedures
Pains
Mental correlation across
two screens
Unfamiliarity with
ultrasound
Steep learning curve
Complication risk
7. We refined surgeons into customer
segments… and value propositions
Field High
volume
procedure
core need currently
uses lap
ultrasound
Does NOT
use robot
Urology partial neph See target and vessels (fast, sans
radiologist, mobile)
⇒ do more laps (vs. open)
✔
Gynecology hysterec-tomies
See the ureter
⇒ fewer complications
no, but can
read it
✔
Oncology liver
resections/
ablations
See the target with ablation needle critical
sections
⇒ fewer readmissions
✔ ✔
Thoracic ? lesion location in collapsed lung
⇒ less invasive (more laps, no hand
port)
no ✔
9. So here’s what we did next:
Experiment: Talk to urologic surgeons (and
oncologic, gynecologic, thoracic)
Insight: Good feedback on MVP from
urologists, but thoracic presented as an even
more compelling opportunity.
10. We kept talking to surgeons - and found patterns in
thoracic surgery
Pains
- Disorienting
- Hour-long search
“Would do anything to
localize tumors minimally
invasively”
11. We kept talking to surgeons - and found patterns in
thoracic surgery
Pains
- Disorienting
- Hour-long search
“Would do anything to
localize tumors minimally
invasively”
50-100 cases a year at academic hospitals
⇒ $250M market opportunity
12. Customer segments - what we learned
(# of people overall supporting)
High volume
procedure
core need uses lap
ultrasound
Does NOT
use robot
Urology partial neph See target and vessels
⇒ do more laps (vs. open) ✔
Gyn hysterectomies
endometriosis?
endomet surgery is sensitive to depth
⇒ provide real-time depth (1mm
accuracy) to prevent uterus
punctures (2)
no, and most
(3) can’t
justify port
small but
growing
Oncology focus on
ablations
Losing cases to interv rads (9)
⇒ tool nav in lap ablation is hard, we
would track everything in one place
✔ ✔
Thoracic VATS for
primary lung
lesions
lesion location in collapsed lung
⇒ less invasive (more laps, no hand
port), easier workflow (no fiducials),
organ sparing, find smaller nodules,
⇒ no reliance on interv rad (12)
no, but willing
to learn (10) limited
14. There were many other learnings...
KP
KA
KR
Luminary
Surgeon
(KOL)
Ultrasound
Company
Lap camera
company
Training Curriculum
Enhancement
Lap Ultrasound
Visualization Studies
Integration
Refinement
Software
Devels APIs OR Access
CR - GET
Conference
Presentations
Youtube
Publications
CS
Society Courses
Centers of
Excellence
Surgeon
OR
Mngr
Value
asmt
App form & pres comm
support
Proforma Financials
Admin
council
Tech
assmnt
committee
Conference
Presentations
Youtube
Publications
VAC
Society Courses
Centers of
Excellence
App form & pres
support
Proforma
Financials
Interest
Consideration
Purchase
Awareness
Booth
Installation at
luminary
sites/KOLs
Keep
Support
Unbundle
Track other tools
Use other
camera/
ultrasound
Upsell
Advanced Viz:
Vessel seg
Advanced Viz:
3D recon
Cross Sell
Other surgeons
(thoracic,
urologic,
oncology, gyn)
Referrals
Academic
hospitals
Main-stream
hospitals
US
comps
Co-sales
IGI Tech
surgns
Tracking
company
OR
Mngers
equipme
nt supply
contract
hospital
profit,
etc.
disposab
lmarkers
profit,
etc.
disposable
markers
15. … and we are in a better position than
ever for commercialization
Pivot:
Away from urology to thoracic
Customer Segments:
Primary - Thoracic
Secondary - Urology, Gynecology, Oncology
U.S. Market Opportunity:
$250 Million
102 Interviews:
55 Surgeons
6 Radiologists
10 Surgical support
10 Hospital administrators
5 Ultrasound company officials
3 Robot company officials
2 Tracking company officials
4 Regulatory, reimbursement, IP specialists
7 Misc
Product: Thoracic surgeons find small-cell
carcinoma lung nodules twice as fast without
preoperative preparation.
info@igitechnologies.com
www.igitechnologies.com
19. With respect to submitting an SBIR/STTR Phase II application, we are making the
following decision (PICK ONE)
● Go with a nominal pivot: The feasibility data generated in the Phase I
grant provide the appropriate technical foundation for a Phase II
application, AND we are largely targeting the customer segments that
we had originally anticipated*
● Go with a significant pivot: The feasibility data generated in the Phase I grant
provide the appropriate technical foundation for a Phase II application, BUT
we are targeting very different customer segments than we had originally
anticipated
● No Go: We do not have a product/market fit that supports the continuation of
this project in its current form, and/or we have made substantial pivots to the
business model that require us to obtain additional technical feasibility data
that should more appropriately be pursued under a new Phase I grant (or
other R&D grant)
● No Go: We plan to continue pursuing this project, but we intend to finance this
project through other non-federal sources (e.g., venture, strategic partner, etc)
*we view our thoracic segment as a refinement of our existing plan, and pivot within the
course
Current
Start
IRL = 6 (soft)
(we have mostly validated 4-6)