Download as PDF, PPTX
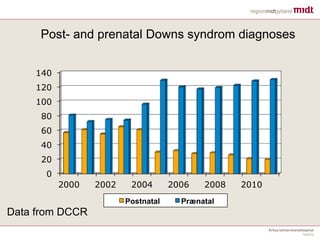

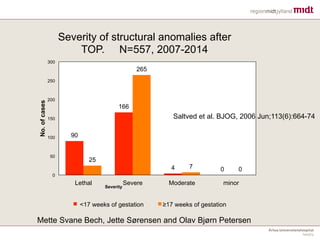
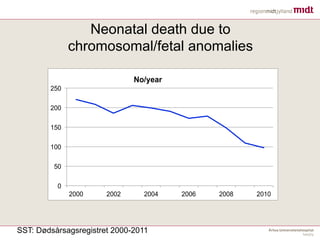
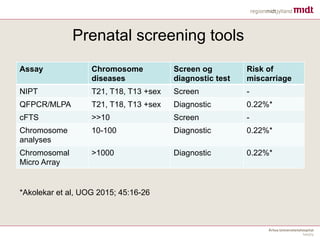
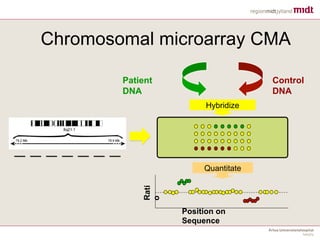
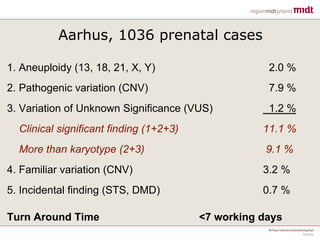
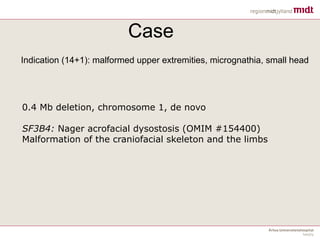

Danish experiences with Chromosomal Micro-Array (CMA) in prenatal settings. Since 2004, all Danish women are offered combined first trimester screening and anomaly scans. The use of CMA in Denmark has increased the detection rate of chromosomal abnormalities compared to traditional chromosome analysis. CMA is now considered the first-tier test for pregnancies with structural malformations, enlarged nuchal translucency, or unexplained growth issues. While CMA provides more information, it also returns more variants of unknown significance which require careful counseling and consideration in pregnancy management decisions.


















































































