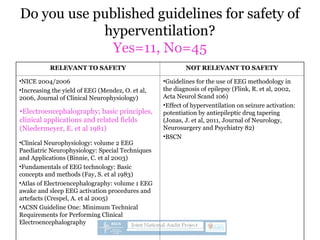
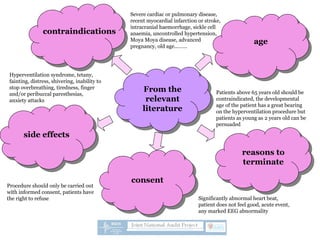
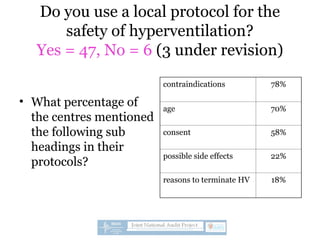
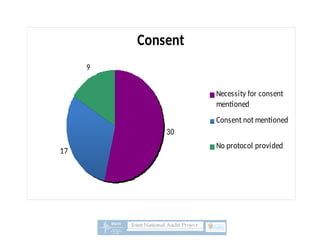
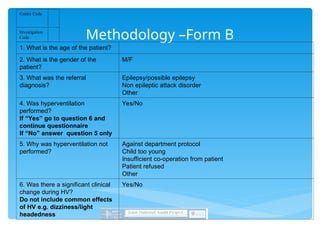
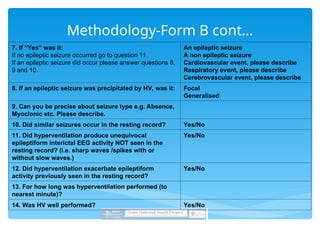
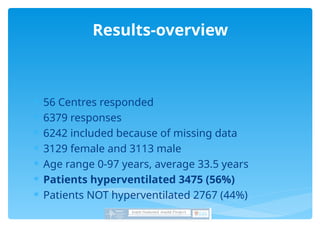
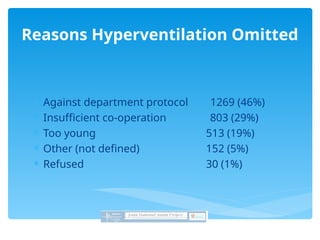
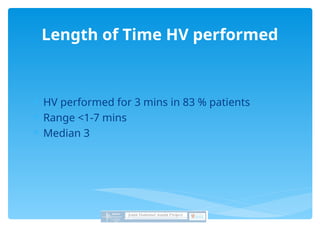
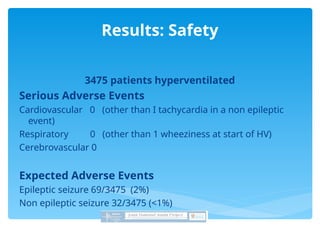
A national survey evaluated the safety and efficacy of hyperventilation during EEG procedures, with a response rate of 89% from 63 forms. Results showed that only 20% of departments utilized published safety guidelines, while 84% had safety protocols addressing age limitations, contraindications, and consent. The survey suggested hyperventilation is generally safe but highlighted the need for more standardized protocols and evidence-based guidelines.







































![MYASTHENIA GRAVIS 33333333333333333[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/myastheniagravisautosaved-250219141012-f3e3b116-thumbnail.jpg?width=640&height=640&fit=bounds)



























