Objective
1. Learn howto measure blood pressure.
2. Interpret blood pressure readings based on
child development.
3. Understand the circumstances of discovery.
4. Comprehend the pathophysiological
mechanisms.
5. Recognize clinical elements.
6. Consider etiology and conduct etiological
assessments.
7. Identify complications.
8. Treat and monitor hypertension.
3.
Childhood Hypertension: Overview
KeyFacts & Prevalence
Risk Factors
Primary Hypertension
• Obesity
• Sedentary lifestyle
• Low birth weight
• Hyperlipidemia
• Family history
• Stress
• Sodium consumption
Secondary Hypertension
• Umbilical artery catheterization
• Urinary infections
• Genetic disease
Note: Younger children with higher blood pressure are
more likely to have secondary causes
• Secondary hypertension is more
common in children than
adults, with an overall
prevalence of around 3.5% in
children and adolescents .
Higher
Prevalence in
Children
• 30% of children with BMI > 95th
percentile have hypertension,
with increasing prevalence due
to the obesity epidemic and
metabolic syndrome
Obesity
Connection
• Early identification and
treatment can significantly
improve long-term
cardiovascular outcomes
Long-term
Impact
4.
Blood pressure isthe force exerted
by blood on the artery walls, defined
by two values:
Systolic Blood Pressure
(SBP): The higher value
during the heart's
contraction phase.
Diastolic Blood Pressure
(DBP): The lower value
during the heart's
relaxation phase.
In 1977, the National Heart Lung
and Blood Institute created a Task
Force on Blood Pressure Control in
Children. The report, revised in 1987
and 1996, defines normal limits
(90th and 95th percentiles) based on
the child's age, gender, and height.
Hypertension is defined
as SBP and DBP above
the 95th percentile for
age, gender, and height
on three successive
measurements.
I. Blood Pressure Definition
Patients
The patient shouldbe relaxed and seated at rest for three to five minutes.
Young children can be comforted by sitting on their parents' lap if
necessary.
It is important to adhere to these conditions to avoid elevated blood
pressure due to isolated consultation hypertension or the "white coat
effect," common in young individuals.
Hypertension diagnosis is confirmed only after three successive readings.
7.
Cuff
The cuff sizeshould match the child's arm size. An undersized cuff will
overestimate blood pressure, while an oversized cuff will underestimate it.
The inflatable part of the cuff should cover 80-100% of the arm circumference midway
between the olecranon (elbow) and the acromion (shoulder). The width should be 40%
of this circumference.
8.
Understanding White CoatBlood
Pressure
White Coat Effect
A temporary increase in blood pressure
that occurs at the start of a medical
consultation
• Blood pressure normalizes after a few
minutes of rest
• Usually triggered by consultation-
induced
• stress
White Coat Hypertension
• Blood pressure remains normal
outside medical settings.
• Requires annual monitoring
outside the medical office.
• Higher risk of developing true
hypertension.
Persistent elevation of
blood pressure during
medical visits:
9.
• The 2017American Academy of Pediatrics (AAP)
guidelines for hypertension in children and
adolescents, endorsed by the American Heart
Association (AHA), recommend:
• For children without risk factors, measure blood
pressure from age three during annual health
check-ups.
• For children aged ≥3 years with hypertension risk
factors, measure blood pressure at every
healthcare encounter (Table 1).
• For children under 3 years with hypertension risk
factors, measure blood pressure at every health
examination (Table 2).
• Children with systolic or diastolic blood pressure
exceeding screening thresholds for their age and
sex (Table 3) require further evaluation, starting
with repeated measurements.
Blood
Pressure
Screening
Normal Blood Pressure Values
10.
Risk Factors forHypertension
in Children ≥3 Years
Check blood pressure at all health visits for children with the following elements:
Medical Conditions
• Type 1 or Type 2 Diabetes
• Kidney disease
• History of obstruction or coarctation of the aortic arch
Physical Factors
• Obesity
Prescription Medications
• Glucocorticoids
• Stimulants
• Tricyclic antidepressants
• Decongestants
• Caffeine
• NSAIDs
• Cocaine
Adapted from: Flynn JT, Kaelber DC, Baker-Smith CM, et al. Clinical practice guideline for screening
and management of high blood pressure in children and adolescents. Pediatrics 2017.
Blood Pressure ClassificationStudy
A study from Nancy, conducted by the Society of Pediatric Nephrology, established blood pressure
classifications based on 17,067 patients (ages 4-18, heights 95-185 cm).
1 Normal Blood Pressure
Below 97.5th percentile
2 Borderline/Moderate
Hypertension
Between 97.5th percentile and
97.5th percentile + 10 mmHg
3 Confirmed Hypertension
Between 97.5th percentile + 10
mmHg and 97.5th percentile + 30
mmHg
4 Immediately Threatening Hypertension
Exceeding 97.5th percentile + 30 mmHg
Special Age Considerations:
• Ages 2-4: Apply criteria for 95 cm height
• Under 2 years: Threshold at 115/70 mmHg
• Newborns: Hypertension starts at 95/65 mmHg
16.
Figure: Blood pressureof boys (A) and girls (B) aged 4 to 18 years based
on height. Study from Nancy and thresholds for hypertension (HTN) by the
Pediatric Nephrology Society.
17.
However, in routinepractice, simple formulas provide
approximately normal values based on the child's age
(Salomon, 2006):
- SBP = 100 + (age x 2)
- DBP < 11 years = 60 + (age x 2)
- DBP > 11 years = 70 + age
• (age expressed in years)
18.
Pathophysiological
mechanism
● Blood pressureis a contributed
of cardiac output and peripheral
vascular resistance.
● Increases in either or both of these
mechanism lead to hypertension.
● Many mechanisms play a role in
primary hypertension: volume
overload (sodium retention, excess
sodium), volume distribution
(sympathetic overcapacity and
renin, stress) and increased
peripheral resistance (renin and
sympathetic activity, insulin,
endothelin).
Volume overload → Increased cardiac output →
Higher BP
Increased peripheral resistance → Higher
afterload → Higher BP
Sympathetic activation → Both increased CO and
PVR
RAS activation → Both volume retention and
vasoconstriction
19.
Clinical
signs
• As inadults, high blood pressure in children
is often asymptomatic
• High blood pressure can be revealed by
minor symptoms:
– Morning headaches, in helmets, sometimes
beating
– unexplained vomiting,
– dizziness,
– cramps,
– impressions of flying flies, visual fog,
– ringing in the ears,
– various paresthesia.
20.
• Polyuro polydipsiasyndrome.
• Hemorrhagic syndrome (epistaxis, pre- or post-operative hemorrhage),
• A break in the growth curve of stature weight,
• Rapid weight loss
• Recurrent facial paralysis
• Hypertensive encephalopathy, marked by intolerable headaches, then
prostration that precedes a coma that worsens rapidly, which is due to
increased intracranial pressure or swelling of the brain due to
hypertension→ The child may have paralysis on one side (hemiparesis),
blindness, and speech disorder.
21.
In the neonatalperiod and in infants under 6 months of age
Hypertension in this age group is often latent (silent)
- Growth Defect: failure to thrive.
- Digestive Disorders: Feeding difficulties, vomiting, irritability.
- Vasomotor Disorders: pallor, cyanosis, poor perfusion, and excessive sweating.
Tachycardia or bradycardia may also be present.
- Severe Presentation: Left Heart Failure and Pulmonary Edema
22.
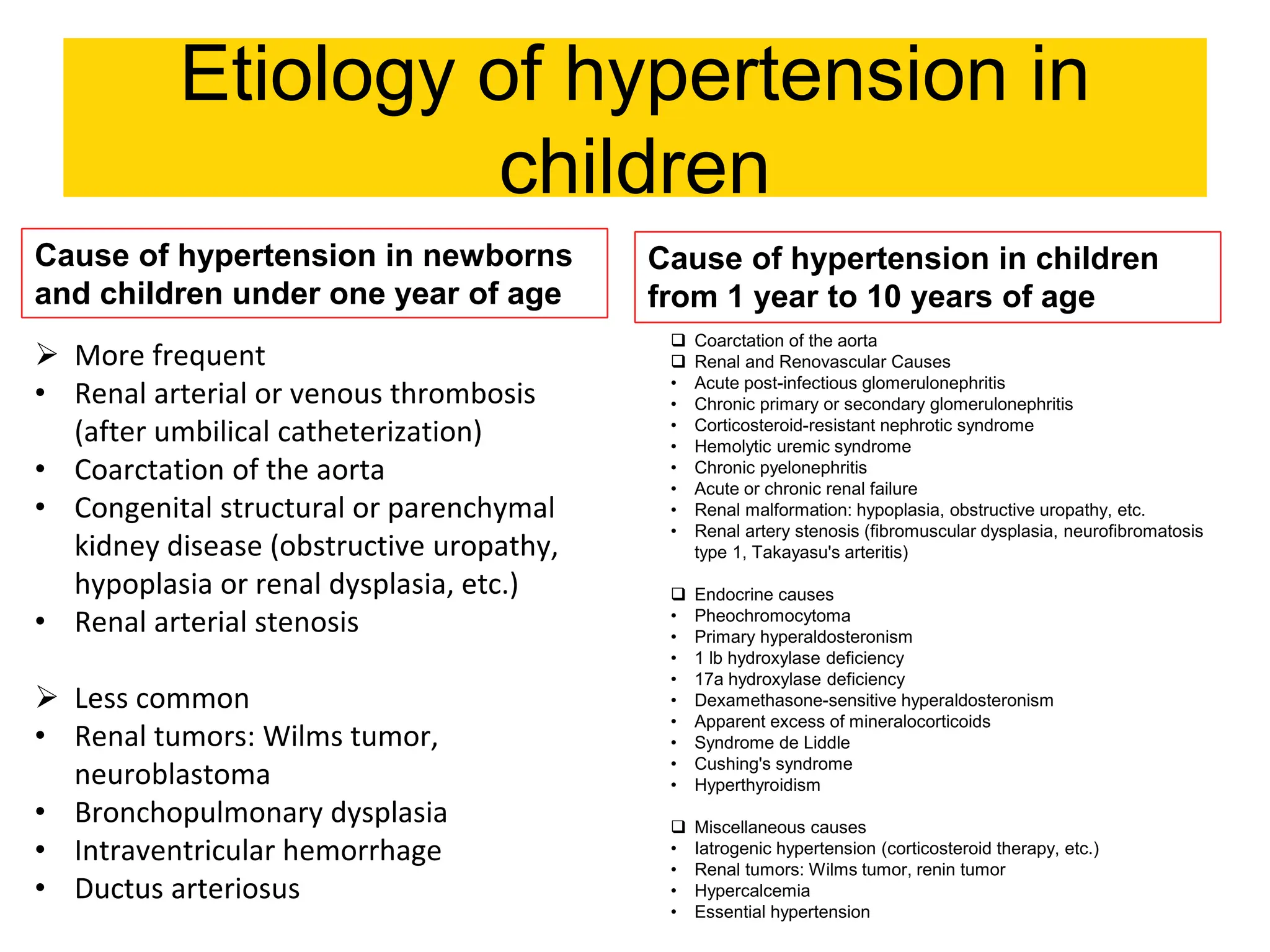
Etiology of hypertensionin
children
Cause of hypertension in newborns
and children under one year of age
Cause of hypertension in children
from 1 year to 10 years of age
More frequent
• Renal arterial or venous thrombosis
(after umbilical catheterization)
• Coarctation of the aorta
• Congenital structural or parenchymal
kidney disease (obstructive uropathy,
hypoplasia or renal dysplasia, etc.)
• Renal arterial stenosis
Less common
• Renal tumors: Wilms tumor,
neuroblastoma
• Bronchopulmonary dysplasia
• Intraventricular hemorrhage
• Ductus arteriosus
Coarctation of the aorta
Renal and Renovascular Causes
• Acute post-infectious glomerulonephritis
• Chronic primary or secondary glomerulonephritis
• Corticosteroid-resistant nephrotic syndrome
• Hemolytic uremic syndrome
• Chronic pyelonephritis
• Acute or chronic renal failure
• Renal malformation: hypoplasia, obstructive uropathy, etc.
• Renal artery stenosis (fibromuscular dysplasia, neurofibromatosis
type 1, Takayasu's arteritis)
Endocrine causes
• Pheochromocytoma
• Primary hyperaldosteronism
• 1 lb hydroxylase deficiency
• 17a hydroxylase deficiency
• Dexamethasone-sensitive hyperaldosteronism
• Apparent excess of mineralocorticoids
• Syndrome de Liddle
• Cushing's syndrome
• Hyperthyroidism
Miscellaneous causes
• Iatrogenic hypertension (corticosteroid therapy, etc.)
• Renal tumors: Wilms tumor, renin tumor
• Hypercalcemia
• Essential hypertension
Coarctation ofthe aorta
– most common cause of hypertension, newborn and infant
– 3M /1F
– Its diagnosis is, in principle, easy and is based on the pulsatile and blood pressure
asymmetry between the upper and lower limbs. The absence of infradiaphragmatic
pulses and more particularly of femoral pulses associated with the presence of a
maximum left laterosternal systolic murmur at the 2nd and 3rd intercostal space with
dorsal irradiation allows in principle a systematic diagnosis from birth.
25.
Nephroblastoma, Wilms tumor
Wilmstumor is a specific kidney
cancer that mainly affects young
children.
It accounts for 5 to 10% of
malignant tumors in children.
It usually develops before the
age of 5 but can sometimes be
seen in older children or even
adults.
They usually have a lump in
the abdomen and may also
suffer from abdominal pain,
high blood pressure, fever, low
appetite, nausea, and vomiting.
26.
hyperthyroidism
• - Thyrotoxicosis
-80% women
- Clinical signs
•
- mercury salt or vapor poisoning
- excess nasal sympathomimetic drugs
• Tachycardia (resting HR persistently >100 bpm)
• Increased systolic blood pressure with wide
pulse pressure
• Palpitations, arrhythmias (e.g., atrial fibrillation,
rare in young children)
• Bounding pulses
27.
Hypertension due toexcess glucocorticoids
• Secondary Cushing's syndrome
• adrenocortical or adrenal carcinoma
ACTH adenoma
Prolonged treatment with high-dose synthetic glucocorticoids
Various causes
• Neurological disorders:
• intracranial hypertension
Guillain and Barré syndrome
acute anterior poliomyelitis
metabolic abnormalities: hypercalcemia, hypercapnia,
porphyria
Poisoning:
• lead poisoning
vitamin D poisoning
28.
Essential arterial hypertensionin pediatrics
• Asymptomatic children
• Progressive rise in blood pressure with age, onset of
hypertension in especially adolescents and pre-
adolescents.
• Systematic blood pressure measurement finds
abnormal figures permanently or intermittently.
• They are often classified as borderline or intermittent
hypertension with numbers above the 95th percentile
but not more than 10 mmHg above this value.
• Eliminate false emotional arterial hypertension in
relation to the doctor's visit.
• Risk factors
• family history of high blood pressure (86%)
• Body mass index greater than the 95th percentile
• absence of sports activity;
• sleep apnea
30.
Clinical Assessment
Family History(ATCD)
• Hypertension or
cardiovascular disease
• Neurological diseases
• Kidney diseases
Personal History (ATCD)
• Neonatal: prematurity, IUGR
• Nephrology: Pyelonephritis
• Current medications
Physical Examination
• Measure height, weight,
and age percentiles
• Blood pressure
measurement in both
arms and leg
• Assessment of femoral pulses
Important Considerations
Leg BP typically 10-20 mmHg higher than arms. Lower leg BP or weak/absent femoral pulses may
indicate aortic coarctation. Obesity has strong correlation with high blood pressure.
Diagnosis
31.
1
Initial Blood Studies
•Complete blood examination (anemia/chronic
kidney disease)
• Fasting blood glucose and lipids
• Electrolyte panel
2 Specialized Blood Analysis
• Kidney function measurements
(urea, serum creatinine)
• Thyroid function (T3, T4, TSH)
3
Urinary Analysis
• Urine sediment analysis
• Dipstick examination
• Proteinuria and hematuria assessment 4 Imaging Studies
• Abdominal ultrasound for kidney cavities and
parenchyma
• Assessment of renal hypoplasia
• Screening for adrenal and retroperitoneal tumors
• Vascular Doppler studies
CT Angiography
Used to search for aortic and renal
stenosis, particularly in cases of
fibromuscular dysplasia
Echocardiography
Serves dual purposes:
•Detection of aortic coarctation
•Exclusion of cardiac etiology and evaluation of left
ventricular hypertrophy as an indicator of long-term
hypertension damage
32.
Complication
• Children andadolescents with severe BP elevation are also at
increased risk of adverse reactions, including hypertensive
encephalopathy, seizures, and even strokes and congestive
heart failure.
• Long-term complications of hypertension are stroke,
cardiovascular impairment resulting in left ventricular
dysfunction/heart failure, kidney failure, and retinopathy
or blindness.
33.
Treatment Approach forPediatric Hypertension
Treatment follows a progressive approach from lifestyle modifications to pharmacological interventions based on severity.
1 Initial Lifestyle Modifications
• Reduce salt intake (<2.5 g/day)
• Increase fresh vegetables, fruits, fiber, and fat-free dairy
• Regular physical activity and sport
• Weight management if obesity present
• Avoid smoke exposure
2 Metabolic Management
Treatment of associated conditions including hyperlipidemia, hypercholesterolemia, and diabetes
3 Immediate Pharmacological Intervention
Required when:
• BP values >95 percentile
• Hypertension is symptomatic (headache, vision disturbance)
• No response to conservative measures
4 Hypertensive Emergency Management
• Treatment via intravenous or oral antihypertensives
• Decrease pressure by 25% or less in first 8 hours
• Gradual normalization over 26-48 hours
• Careful monitoring to prevent rapid reduction and poor organ perfusion
Note: During emergency treatment, simultaneous investigation of underlying causes must be initiated for targeted treatment.
Treatment
34.
Drug treatment
Pharmacological treatmentshould be initiated immediately
in a child with blood pressure values > 97.5 percentile +
30 mm Hg, if the HBP is symptomatic (headache, vision
disturbance), or if the child does not respond to
conservative measures.
Hypertensive emergencies can be treated with either
intravenous or oral antihypertensives, depending on the
child's symptomatology, aiming to decrease the pressure
by 25% or less during the first 8 hours after symptoms
and then gradually normalize BP over 26-48 hours.
Very rapid reduction can lead to poor perfusion of the
brain, coronary arteries, kidneys, etc.
Référence
1. Mattoo, T.K. Definition and diagnosis of hypertension in children and adolescents - UpToDate. UpToDate
1–34 (2019).
2. Pédiatrie, Collection Med-Line.Hypertension Artérielle.
3. JL André, Hypertension artérielle chez l'enfant, ENCYCLOPÉDIE MÉDICO-CHIRURGICALE.
4. B. Fiquet-Kempf, P. Niaudet. hypertension artérielle de l'enfant. J Pédiatr Puériculture 2001 ; 14 : 25-34.
5. Marc B. Lande. Systemic Hypertension. Nelson TEXTBOOK of PEDIATRICS EDITION 20.
6. Pediatric Hypertension, Second Edition, edited by Joseph T. Flynn, MD, MS, Julie R. Ingelfinger, MD, and
Ronald J. Portman, MD, 2011
7. Victoria F. Norwood. Hypertension. Pediatrics in Review Vol.23 No.6 June 2002.
8. The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and
Adolescents. PEDIATRICS Vol. 114 No. 2 August 2004.
9. Leonard G. Feld. Hypertension in Childhood. Pediatrics in Review Vol.28 No.8 August 2007.
10. François Cachat. Traitement de l'hypertension artérielle chez l'enfant: recommandations actuelles.
PAEDIATRICA Vol. 15 No. 5 2004.
11. Tammy M. Brady. Hypertension. Pediatrics in Review Vol.33 No.12 December 2012.




















![Nephropathy
• most common cause of hypertension
• chronic acquired or hereditary
glomerulopathy (Berger, Rheumatoid
Purpura, Alport, etc.)
• autoimmune diseases (systemic lupus
erythematosus, Wegener's disease (anti-
neutrophil antibodies [ANCA]))
• Post-Infectious AGN [GNAPS]
• SHU
• nephrotic syndromes (corticosteroid-resistant
form)
• Polycystic hepatorenal cystic disease.
Purpura
rheumatoid
skin rash
Acute lupus: edematous
erythema in Vespertilio](https://image.slidesharecdn.com/hypertensioninchildren-2025-compressed-250429073326-b92f3cba/75/Hypertension-in-Children-2025-compressed-pdf-23-2048.jpg)
















































![2. traumatisme thoraciques cours 5A.M [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/2-250430155748-b5c38b46-thumbnail.jpg?width=640&height=640&fit=bounds)
































