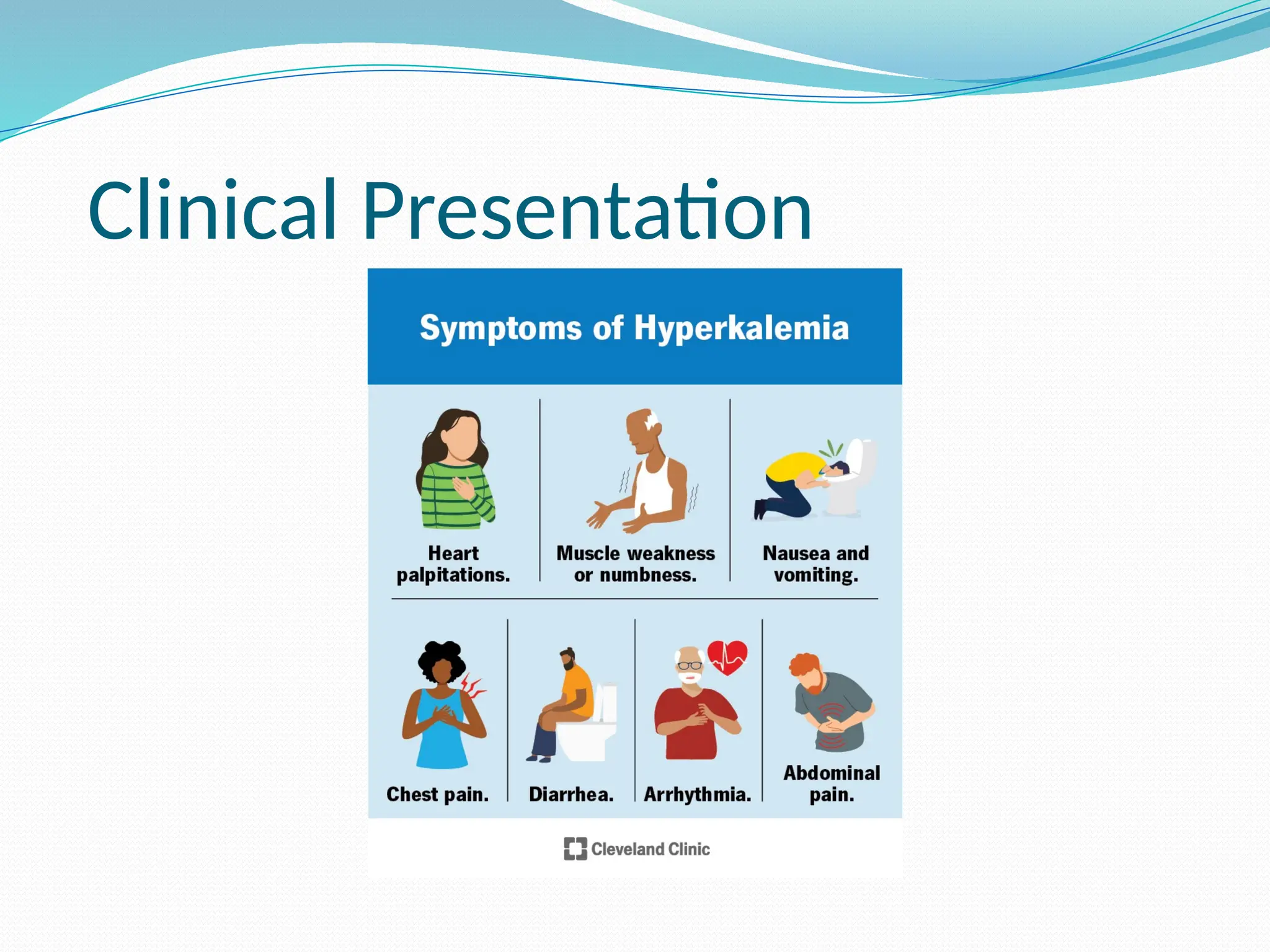
DEFINITION
It is definedas serum potassium concenteration
of greater than 5.5 mEq/L.
The normal concenteration of serum potassium
range from 3.5-5.o mEq/L.
Step 1 –Cardiac Stabilization
Iv 1oml of 10% calcium gluconate
Route slow intravenous push over 2-5 mins with
cardiac monitoring.
Onset: Immediate
Duration: ~30–60 min
Stabilizes myocardium
11.
Step 2 –Shift K+ Intracellularly
10 units of regular Insulin Iv + 25 g of Dextrose
given as:
5oml of 50% dextrose
100ml of 25 % dextrose
25oml of 10 % dextrose
500ml of 5% dextrose
Insulin transpots about 0.6 to 1.2 mEq/L of
potassium.
Sodium Bicarbonate
Dose :50–100 mEq IV
Commonly: 50 mEq in 50 mL of D5W (or sterile
water)
Route: IV over 5–10 minutes (can also be infused
over 30–60 min)
May be repeated based on ABG results and
potassium levels
14.
Step 3 –Eliminate Potassium
Loop diuretics (furosemide)
Dose: 20 mg to 40 mg iv
40 mg to 80mg po
Onset: 5 mins iv
30 – 60 min
Duration: 4-6 hours
Thiazide diuretics ( hydrochlorthiazide)
Dose: 12.5-25 mg orally once daily
15.
Cation exchangeresins ( sodium polyesterene
sulfonate)
Dose: 15 – 60 g orally four times a day
30 – 50 g per rectal every six hourly
Onset: 2-6 hours
Duration: 4-6 hours
Hemodialysis
Hyperkalemia more than 6.5 with Ecg changes
not responding to medical therapy.