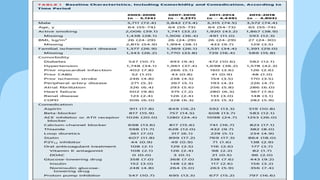
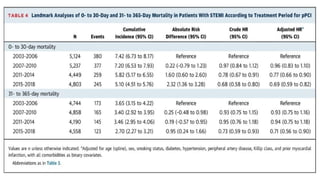
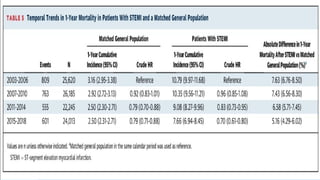
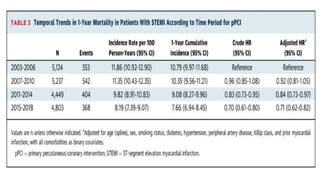
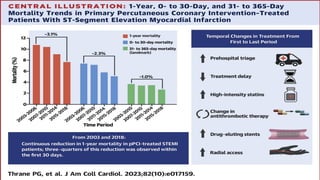
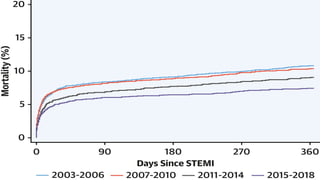
A cohort study conducted in Denmark from 2003 to 2018 examined mortality trends after primary percutaneous coronary intervention (PPCI) for ST-elevation myocardial infarction (STEMI). It found a significant decrease in 1-year mortality rates, dropping from 10.8% to 7.7%, with the most remarkable reduction occurring within the first 30 days post-intervention. Key factors contributing to this decline included improved treatment delays, increased use of drug-eluting stents, and the adoption of newer antiplatelet medications.






































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
