Download to read offline
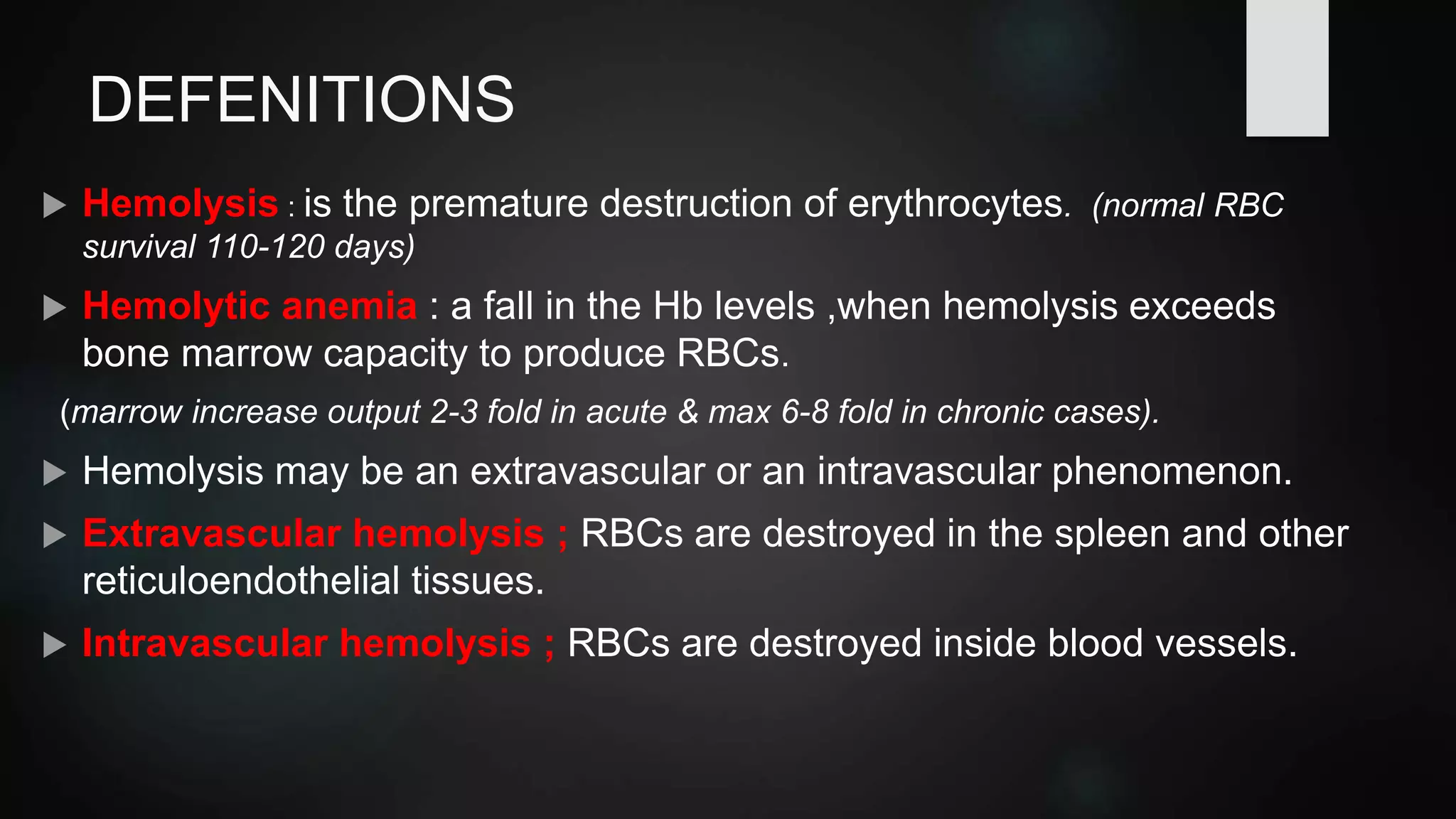
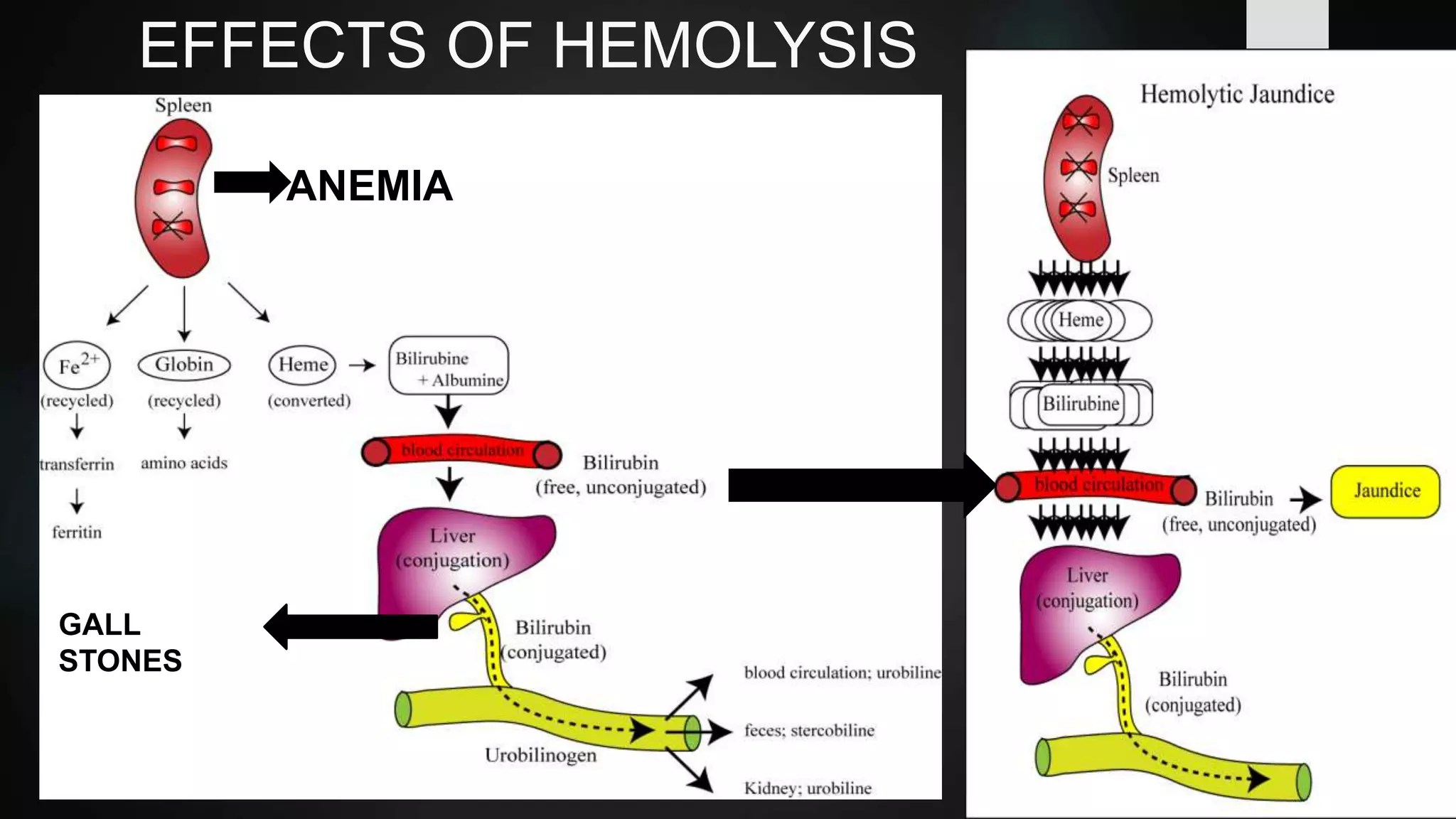
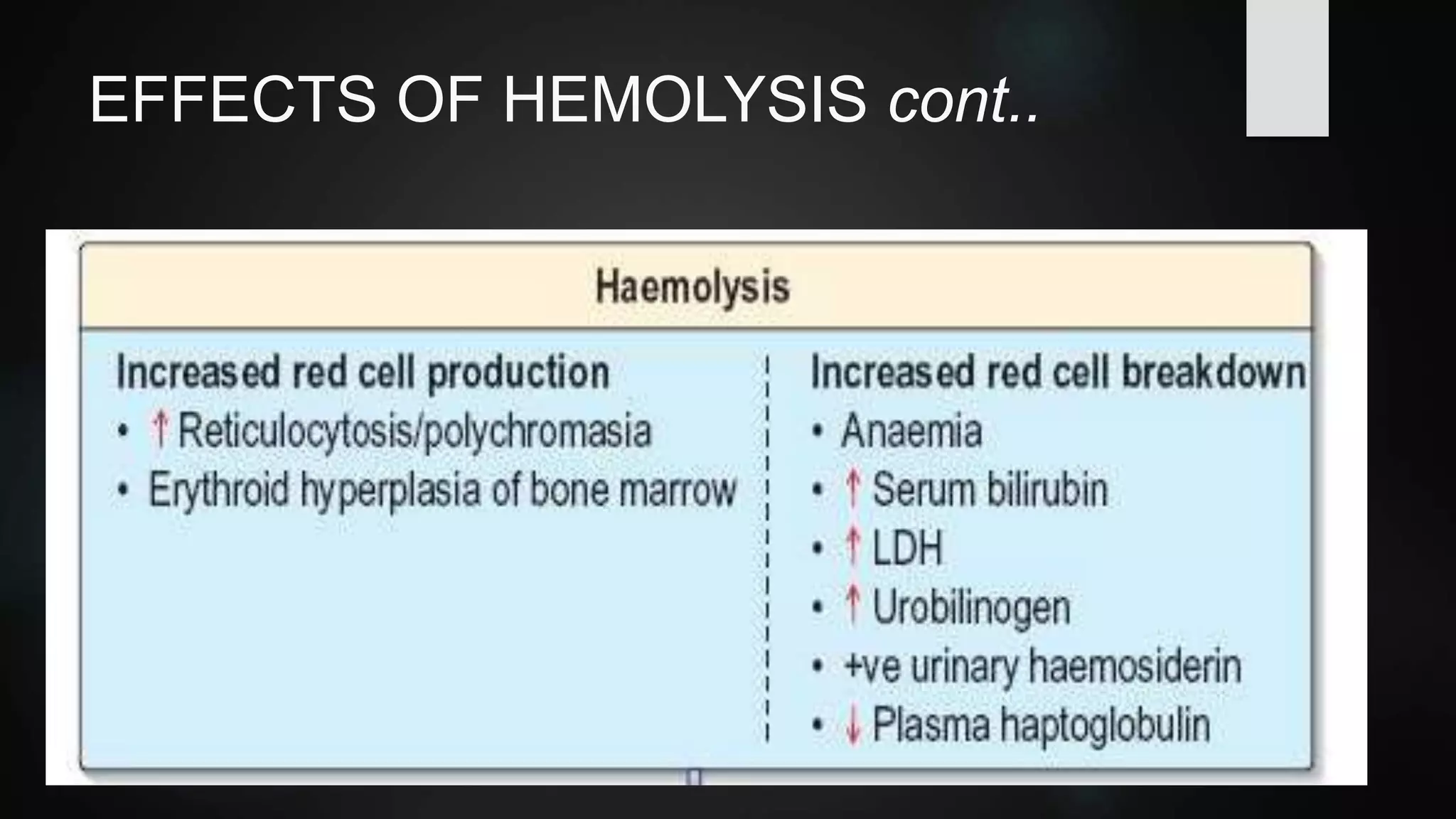
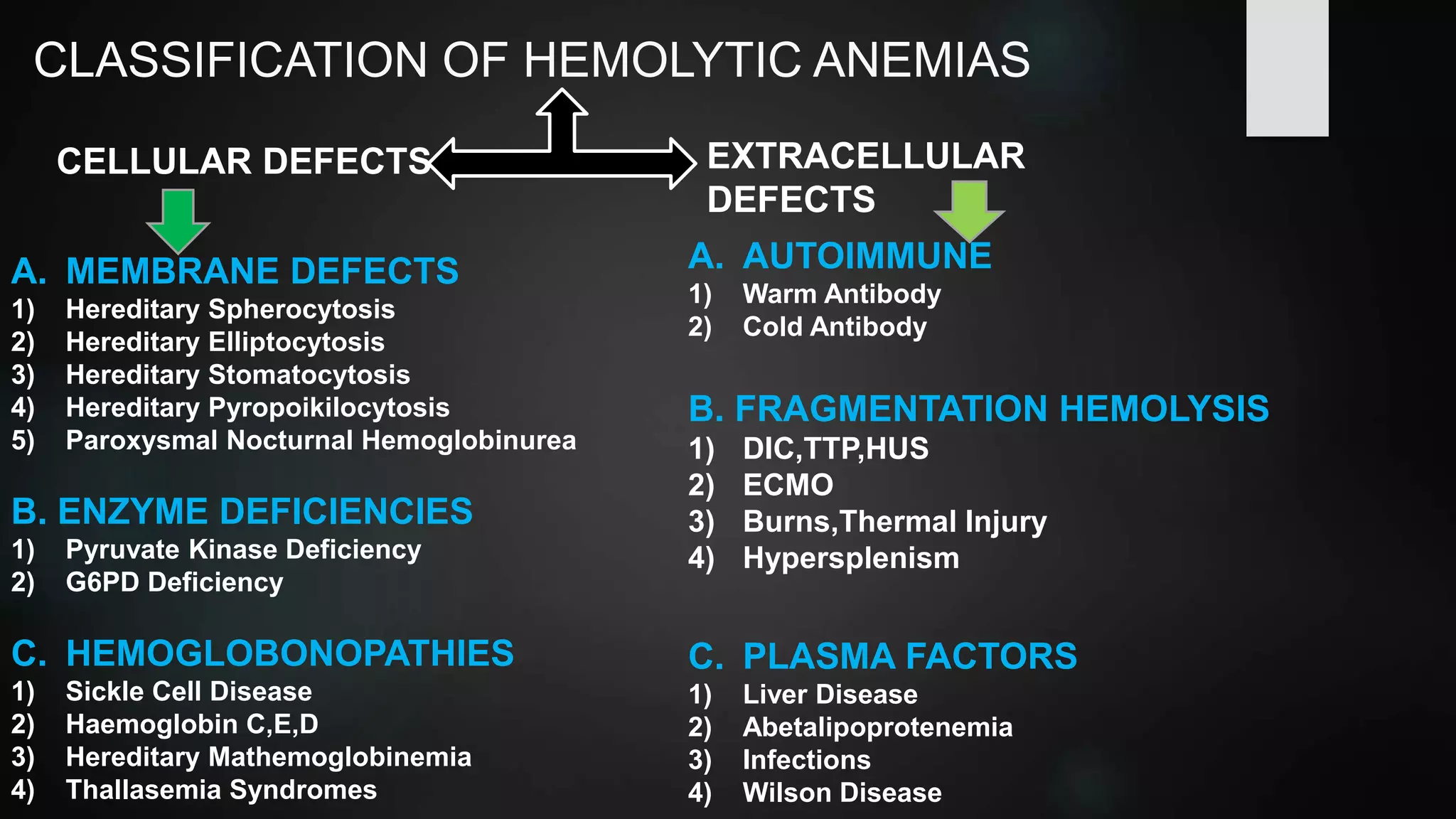


This document defines hemolytic anemias and classifies them based on cellular and extracellular defects. Hemolytic anemia occurs when red blood cell destruction exceeds bone marrow's ability to produce more cells. Destruction can be extravascular, in the spleen, or intravascular, inside blood vessels. The document then focuses on hereditary spherocytosis, a common inherited red blood cell membrane defect where mutations lead to spherical red blood cells that are trapped and destroyed in the spleen, causing hemolysis and anemia.



































































