
![Patient organisations are ideal honest brokers
and custodians in data governance
Patient organisations…
are the ideal custodians on data governance (consent management, collection, data management, ownership,
security)
can enable all stakeholders on purposeful research without compromising patients’ privacy, preventing misuse
can ensure that research results are published irrespective of whether results are positive or negative
may even act as a cooperative or patient-led data commons to collect personal data, and agree that their
pseudonymized personal data is shared as a fiduciary with patient advocacy, academic, pharma or healthcare
system research
MIDATA.coop, POSMO.coop and similar data cooperatives as pilots and a model? Adapted from Prof. Ernst Hafen, ETH Zürich (2021)
Data Commons
[Pseudonymized data
of community members]
clinical medical genomic
PRO
sensors geolocation microbiome
preferences
Patient organisation
Clinical
researchers
Healthcare
providers
Industry
Regulators
Payers
Policy
makers](https://image.slidesharecdn.com/20230503healthdatasharingfrompatientsperspectiveipposi-a-230525080759-e8823bac/75/Health-data-sharing-from-patients-perspective-5-2048.jpg)



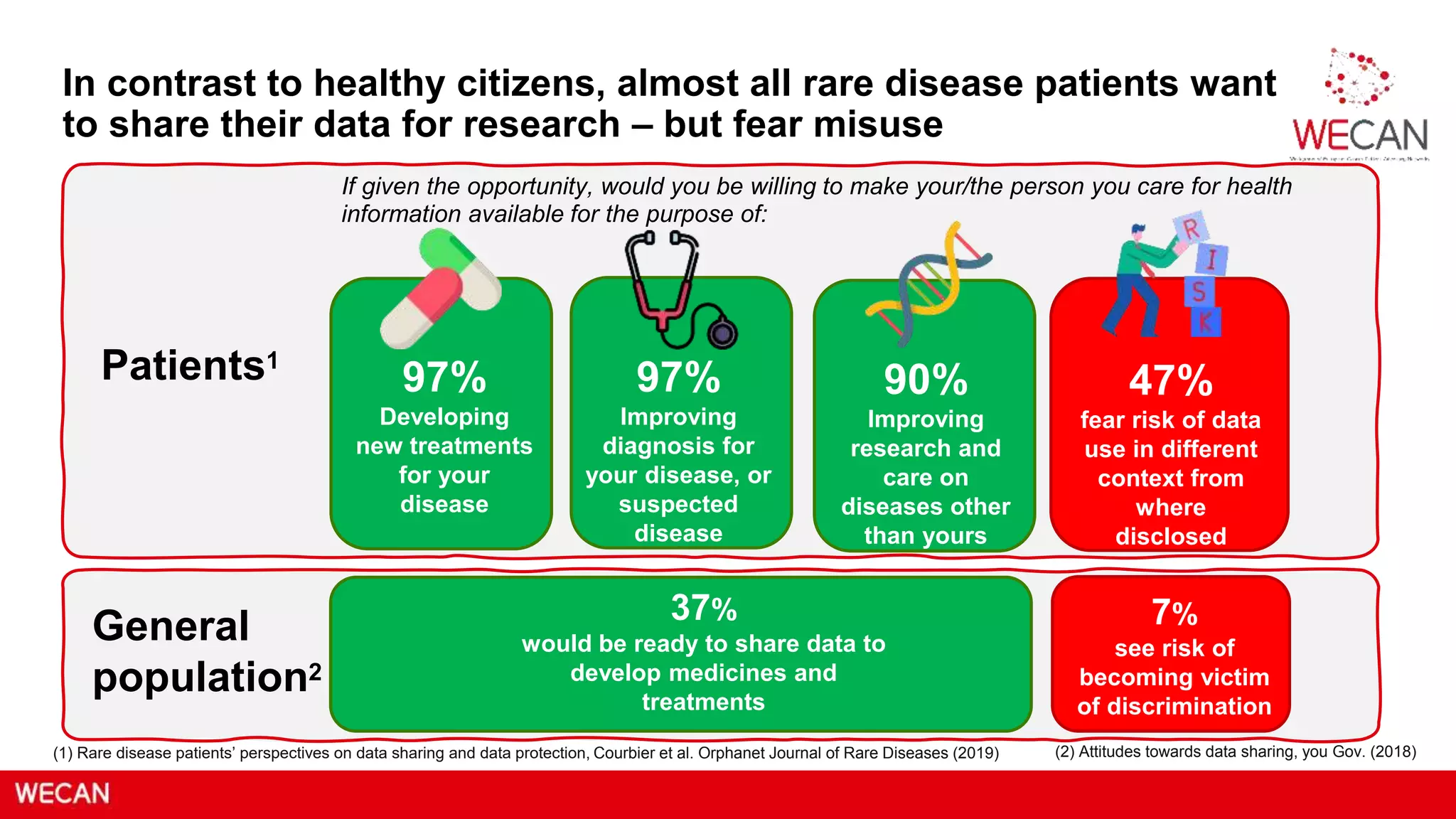
Rare disease patients are eager to share their data for research but are concerned about misuse and discrimination. The GDPR presents an opportunity for better data governance and consent management, with patient organizations acting as trustworthy custodians. These organizations can facilitate ethical research by ensuring patient privacy while providing valuable insights for medical advancements.