Introduction
• Headache isamong the most common reasons patients seek
medical attention.
• The observed 1-year prevalence of any headache was
63.9 %, with a female preponderance of 4:3.
Ref: Kulkarni, G.B., Rao, G.N., Gururaj, G. et al (2015).
3.
•The prevalence ofheadache in Indian population were
found to be 438.8 per 1,000 population (95% CI:
287.6–602.3) (P < 0.0001, I2 = 97.99%)
Ref: Dhiman V et al (2021).
4.
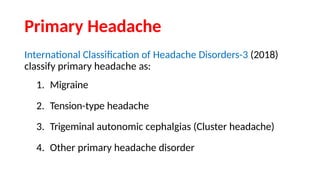
• International HeadacheSociety characterizes headache as:
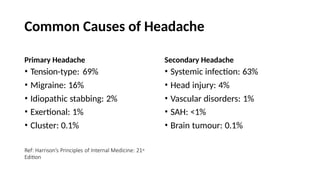
A. Primary Headache
B. Secondary Headache
Ref: International Headache Society 2018
Migraine
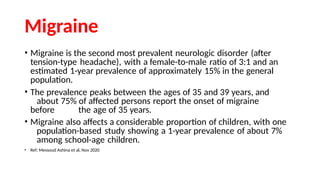
• Migraine isthe second most prevalent neurologic disorder (after
tension-type headache), with a female-to-male ratio of 3:1 and an
estimated 1-year prevalence of approximately 15% in the general
population.
• The prevalence peaks between the ages of 35 and 39 years, and
about 75% of affected persons report the onset of migraine
before the age of 35 years.
• Migraine also affects a considerable proportion of children, with one
population-based study showing a 1-year prevalence of about 7%
among school-age children.
• Ref: Messoud Ashina et al, Nov 2020
Classification as perICHD-3
• Migraine without aura
• Migraine with aura
• Chronic Migraine
• Complications of Migraine
• Probable migraine
• Episodic syndromes that may be associated migraine
Aura
• Early symptomsof an attack of migraine with aura, believed
to be the manifestations of focal cerebral dysfunction.
• The aura typically lasts 20-30 minutes and precedes the
headache.
13.
• Visual aurais the most common type of aura, often
presenting as fortification spectrum (angulated, arcuate and
gradually enlarging visual disturbance typical of
migrainous visual aura, which can be coloured or
black-and-white).
• Sensory disturbances are next among the frequent types of
aura experienced, speech disturbances are less frequent.
Ref: International Headache Society 2018
14.
Chronic Migraine
• Headacheoccurring on 15 or more days/month for more than 3 months,
which, on at least 8 days/month, has the features of migraine headache
• The characteristics of the headache may change not only from day to day but
even within the same day.
• Attacks with and those without aura are both counted, as are both migraine-
like and tension-type-like headaches (but not secondary headaches).
• The most common cause of symptoms suggestive of chronic migraine is
medication overuse.
Ref: International Headache Society 2018
15.
Management of Migraine
•Non-Pharmacologic Management
• Acute Attack Management
• Preventive Treatment
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
16.
Non-Pharmacologic Management
• Identifyingtriggers and avoiding them.
• Regulated lifestyle including a healthy diet, regular exercise,
regular sleep patterns, avoidance of excess caffeine and
alcohol, and avoidance of acute changes of stress levels.
• For most patient, this approach is, at best, an adjunct to
pharmacotherapy.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
17.
Migraine Triggers
• Glare,bright lights, sounds.
• Hunger
• Let-down from stress, physical exertion
• Stormy weather or barometric pressure changes
• Hormonal fluctuations during menses
• Lack of or excess sleep
• Alcohol intake
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
18.
Management of AcuteAttacks
1. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs):
• Acetaminophen- 500 mg q6h
• Ibuprofen- 400 mg po q3-4h
• Acetylsalicyclic Acid (Aspirin)- 500 mg q6h
• Naproxen- 220-550mg po bid
• Antiemetics: Metoclopramide 5-10 mg/d or Domperidone 10 mg
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
19.
• NSAIDs aremost effective when taken early in the migraine attack.
Both severity and duration of an attack can be reduced significantly.
• However, effectiveness of these agents in migraine is usually less than
optimal in moderate or severe attacks.
• FDA approved combination for treatment of mild to moderate
migraine: Acetaminophen, aspirin and caffeine.
• Side effects of NSAIDs include dyspepsia and gastrointestinal
irritation.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
20.
• Contraindications ofNSAIDs:
• Do not use right before or after coronary artery bypass graft.
• Do not use in case of hypersensitivity reaction to NSAIDs.
• Avoid in 3rd trimester of pregnancy.
• Use with caution in patients with peptic ulcer and along with
anticoagulants.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
21.
2. Triptans: 5-HT1B/1DReceptor Agonists
• Oral :
• Sumatriptan- 50-100 mg at onset
• Rizatriptan- 5-10 mg at onset
• Zolmitriptan- 2.5 mg at onset
• Naratriptan- 2.5 mg at onset
• Subcutaneous Sumatriptan 4-6 mg for rapid relief.
(FDA approved)
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
22.
• Triptans aregenerally not effective in migraine with aura unless given
after the aura is completed and the headache initiated.
• Triptans generally does not result in rapid, consistent and complete
relief of migraine in all patients.
• Recurrence of headache, within the usual time course of an attack is
another limitation of triptan use.
• Evidence from RCTs shows that coadministration of longer acting
NSAID, Naproxen 500 mg, with Sumatriptan will augment the
initial effect of Sumatriptan and reduce rates of headache
recurrence.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
23.
• Contraindications ofTriptans:
• In patients with a history, symptoms, or signs of ischemic cardiac, cerebrovascular, or
peripheral vascular syndromes,
• Severe hepatic or renal failure,
• Age of 65 years or more,
• All triptans, except for sumatriptan, are contraindicated in pregnancy and
breastfeeding.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
24.
Preventive Treatments forMigraine
• When to consider?
• Increasing frequency of migraine attacks or with attacks that are either unresponsive or poorly
responsive to abortive treatments.
• Four or more attacks a month.
• Recurrent migraine attacks are causing considerable disability despite optimal acute drug
therapy
• Frequency of acute medication use is approaching levels that place the patient at risk of
medication-overuse headache.
• Contraindications to acute migraine medications are making symptomatic treatment of migraine
attacks difficult.
25.
• Beta-blockers :
•Propranolol, atenolol, and metoprolol
• Contraindicated in patients with asthma, chronic obstructive pulmonary
disease, insulin-dependent diabetes mellitus, heart block or
failure, or peripheral vascular disease.
• Propranolol can be started in a dose of 10 mg twice daily and gradually
increased to a maximum of 80-120 mg per day.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
26.
• Calcium channelblockers :
• Flunarizine is most commonly used for migraine prophylaxis.
• Dose – 5-15 mg/d
• Flunarizine is to be avoided in patients with depression.
• Calcium-channel blockers are contraindicated in patients with hypotension,
congestive heart failure, or arrhythmia.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
27.
• Tricyclic antidepressants:
•Amitriptyline is useful in migraine, especially in patients with
associated TTH
• Dose- 10-75 mg/ day
• Contraindications include cardiac, kidney, liver, prostate and thyroid disease,
glaucoma, hypotension, seizure disorder, and use of monoamine
oxidase inhibitors.
• Use with caution in elderly.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
28.
• Anti-epileptics :
•Valproate and Topiramate have been found to be effective for migraine
prophylaxis.
• Should not be given to women who are pregnant or considering
pregnancy or young women with polycystic ovarian disease (PCOD).
• Valproate: 400-600 mg bid
• Topiramate: 25-200mg/d
29.
• Topiramate hasthe advantage of weight loss and can be used in
preference to divalproex when treating obese patients.
• Topiramate should not be used in the presence of glaucoma and
renal stones.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
30.
Treatment in PregnantWomen
• Paracetamol should be used as the first-line medication for acute
treatment of migraine in pregnancy.
• NSAIDs can be used only during the second trimester.
• Triptans should be used only under the strict supervision of a
specialist, as the safety data available are limited and originate from
post-marketing surveillance; most data relate to the use of
sumatriptan.
• For nausea associated with migraine in pregnancy, metoclopramide
can be used.
31.
• Preventive migrainemedications are best avoided during pregnancy
owing to the potential for fetal harm. However, if preventive
therapy is considered clinically indicated because of frequent
and disabling migraine attacks, the best available safety data
support the use of propranolol or, if propranolol is contraindicated,
amitriptyline.
• Topiramate and sodium valproate are contraindicated.
• Migraine medication therapy in the post-partum, Paracetamol is the
preferred acute medication, although ibuprofen and sumatriptan are
also considered safe. If preventive medication is required,
propranolol is the recommended first choice as it has the best safety
profile.
Ref: Anna K. Eigenbrodt et al, 2021
32.
Treatment in Womenwith menstrual
migraine
• Women with migraine experience migraine attacks that are
exclusively related to their menstruation, referred to as pure
menstrual migraine.
• If optimized acute medication therapy does not suffice for these
patients, initiation of perimenstrual preventive treatment should be
considered.
• A long-acting NSAID (naproxen) or triptan for 5 days, beginning 2 days
before the expected first day of menstruation.
33.
• Some womenwith pure menstrual migraine without aura benefit
from continuous use (that is, without a break) of combined hormonal
contraceptives.
• By contrast, combined hormonal contraceptives are contraindicated
in women with migraine with aura regardless of any association
with their menstrual cycle, owing to an associated increase in the
risk of stroke.
Ref: Anna K. Eigenbrodt et al, 2021
34.
Migraine in Childrenand Adolescents
• Ibuprofen is considered the initial drug of choice.
• If ibuprofen is ineffective, oral triptans and the combination of
sumatriptan and naproxen sodium may be tried.
• There is less evidence supporting the use of preventive medications,
such as topiramate, amitriptyline, and propranolol in children and
adolescents. In a placebo-controlled trial, topiramate and
amitriptyline were not superior to placebo for the prevention of
migraine in patients 8 to 17 years of age.
• Children and adolescents may benefit from biobehavioral therapies,
such as biofeedback, relaxation, and cognitive behavioral therapy.
Ref: Messoud Ashina et al, Nov 2020
35.
Newer Therapies
• CalcitoninGene-Related Peptide (CGRP) Receptor Antagonists, aka
Gepants are effective in acute treatment of migraine.
• Rimegepant and Ubrogepant are approved by FDA. Both are likely to
render patients pain-free at 2 hours.
• Monoclonal antibodies targeting CGRP for prophylactic use.
36.
• Four monoclonalantibodies to CGRP or its receptor have been shown to be
effective in migraine prevention-
1. Galcanezumab (240 mg subcutaneous, then 120 mg subcutaneous once
monthly),
2. Eptinezumab(100 or 300 mg intravenous quarterly),
3. Erenumab(70 or 140 mg subcutaneous once monthly), and
4. Fremanezumab(225 mg subcutaneous once monthly or 675 mg
subcutaneous once quarterly).
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
Ref: Anna K. Eigenbrodt et al, 2021
37.
• 5-HT1F ReceptorAgonists, Lasmiditan, has been approved by FDA for
acute treatment of migraine.
• These have no vascular effects, hence can be used safely in patients
with cardiovascular and cerebrovascular disease.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
38.
Neuromodulation
• Single-pulse transcranialmagnetic stimulation (sTMS) is
FDA approved for acute treatment (4-24 pulses per day).
• A noninvasive vagus nerve stimulator (nVNS) is FDA approved for
treatment of migraine (one to two 120 sec doses).
• Remote electrical neuromodulation using a smartphone app that
stimulates the upper arm for 30-45 minutes is also FDA approved for
acute migraine.
• Transcutaneous supraorbital nerve stimulation for 60 minutes is also
FDA approved.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
39.
Ref: Messoud Ashinaet al, Nov 2020
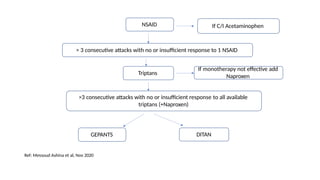
NSAID
> 3 consecutive attacks with no or insufficient response to 1 NSAID
Triptans
>3 consecutive attacks with no or insufficient response to all available
triptans (+Naproxen)
GEPANTS DITAN
If C/I Acetaminophen
If monotherapy not effective add
Naproxen
40.
• Antiemetic agentsmay be offered as adjunctive therapy in patients
with attacks accompanied by nausea or vomiting.
• Initiation of preventive treatment should, in general, be considered
for patients who have at least 2 migraine days per month and are
adversely affected despite therapy.
Ref: Messoud Ashina et al, Nov 2020
41.
Tension Type Headache
•Very common, with a lifetime prevalence in the general population
ranging between 30% and 78%.
• More common in women than men.
Ref: ICHD-3, 2018
Chronic Tension-type Headache
•Headache occurring on ≥15 days/month on average for >3 months
(≥180 days/year)
• Episodes of headache, typically bilateral, pressing or tightening in
quality and of mild to moderate intensity, lasting hours to days, or
unremitting.
• The pain does not worsen with routine physical activity, but may be
associated with mild nausea, photophobia or phonophobia.
• In many uncertain cases there is overuse of medication.
Ref: International Headache Society 2018
46.
• Similar tothe association between migraine and psychiatric disorders,
tension-type headache, especially chronic TTH, is strongly associated
with GAD and MDD.
• Generalized anxiety was found to be present in 38.5%-52.5% of TTH
patients.
• Additionally, major depression is also found frequently in
patients with TTH (32.7%-36.4%).
• Finally, suicidal ideation may be associated with TTH disorders. In a
recent study, 17.3% of TTH sufferers reported suicidal ideation.
Ref: International Headache Society 2018
47.
Management of TTH
•Acute abortive treatment
• Simple analgesics and NSAIDs are the mainstays in the acute therapy.
• Preventive treatment:
• Tricyclic antidepressants: Amtriptyline has been found to be most effective,
should be started on low dose (10 mg to 25 mg per day) and titrated by
10-25 mg weekly till the therapeutic effect or the side effects appear
• Mirtazapine upto 30 mg/day can be given as second line.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
48.
Non- Pharmacological Managementof TTH:
• Relaxation training :
The goal is to help the patient to recognize and control tension as
it arises in the course of daily activities.
During the training, the patient sequentially tenses and then
releases specific groups of muscles throughout the body.
49.
• EMG biofeedback:
The aim is to help the patient to recognize and control muscle
tension by providing continuous feedback about muscle activity.
Sessions typically include an adaptation phase, baseline phase,
training phase where feedback is provided, and a self-control phase
where the patient practices controlling muscle tension without the
aid of feedback
50.
• Cognitive-behavioural therapy:
The aim of cognitive-behavioural therapy is to teach the patient
to identify thoughts and beliefs that generate stress and aggravate
headaches.
These thoughts are then challenged, and alternative adaptive
coping self-instructions are considered.
51.
A varietyof exercises may be used to challenge thoughts and beliefs,
including experimenting with the adoption of another person's view
of the situation, actively generating other possible views of a
situation, and devising a behavioural experiment to test the validity of
a particular belief.
• Physical therapy : includes the improvement of posture, relaxation,
exercise programs, hot and cold packs, ultrasound and electrical
stimulation.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
52.
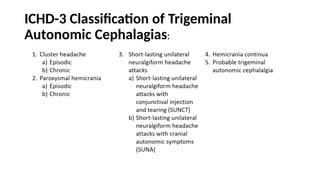
Trigeminal Autonomic Cephalalgias
•The incidence of TACs is low, with Cluster Headache being the most
common with a prevalence of approximately 0.1% of the population
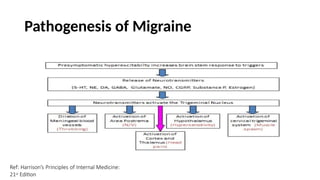
• Simultaneous activation of the trigeminal system and of the
autonomic nervous system is a common feature of all trigeminal
autonomic cephalalgias
• Produces the clinical picture of short-lasting, strictly
unilateral headache attacks with ipsilateral autonomic
symptoms.
Ref: International Headache Society 2018
Cluster Headache
• Ageat onset is usually 20-40 years.
• Men are afflicted three times more than women.
• Can be episodic or chronic.
• About 10-15% of patients have Chronic cluster headache
55.
• Cluster headacheis maximal orbitally, supraorbitally, temporally or in
any combination of these sites, but may spread to other regions.
• During the worst attacks, the intensity of pain is excruciating. Patients
are usually unable to lie down, and characteristically pace the floor.
Pain usually recurs on the same side of the head during a single
cluster period.
• Acute attacks involve activation in the region of the posterior
hypothalamic grey matter.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
• Attacks occurin series lasting for weeks or months (so-called cluster
periods or bouts) separated by remission periods usually lasting
months or years.
• Chronic cluster headache : Cluster headache attacks occurring for
one year or longer without remission, or with remission periods
lasting less than 3 months.
58.
• Cluster Headacheare primary in nature, but may be a rare
manifestation of an underlying space-occupying lesion, (especially
pituitary tumors)
• Hence neuroimaging studies of all cases of CH are recommended.
• Treatment includes abortive treatment for acute attacks and
preventive treatment.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
59.
Abortive Treatment
• SCSumatriptan: Given as 6 mg SC injection OR
• Intranasal Sumatriptan (20 mg) or Zolmitriptan (5mg)
• Oxygen: Inhalation of 100% oxygen at 6-7 L/min for 15 min is effective
in 60% cases. Higher flow rate (12 L/min) may benefit some patients
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
60.
Preventive Treatment
• Verapamil:
•Pretreatment ECG is essential and this drug should be avoided in conjunction
with betablockers.
• It is given in a starting dose of 120 mg long acting daily increased to three
times
daily.
• Lithium:
• Precheck of thyroid and renal profile is necessary and lithium levels need to be
monitored periodically.
• Given in a starting dose of 300 mg to be gradually increased to a maximum of
900 mg.
• Steroids: Prednisolone in a dose of 60 mg daily to start with followed by gradual
tapering.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
61.
Medication Overuse Headache
•Overuse of analgesic medication for headache can aggravate
headache frequency, markedly impair the effect of preventive
medicines, and induce a state of refractory daily or near-daily
headache.
• Substantial improvement in severity and frequency after cessation of
analgesics.
• Reduce the medication dose by 10% every 1-2 weeks.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
62.
• Be alertto the possibility of medication overuse headache in people
whose headache developed or worsened while they were taking the
following drugs for 3 months or more:
• triptans, opioids, ergots or combination analgesic medications on
10 days per month or more or
• paracetamol, aspirin or a shorter-acting NSAIDs, either alone or in
any combination, on 15 days per month or more
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
63.
• Diagnostic criteria(ICHD-3):
A. Headache occurring on 15 days/month in a patient with a pre-
existing headache disorder
B.Regular overuse for >3 months of one or more drugs that can
be taken for acute and/or symptomatic treatment of headache
C. Not better accounted for by another ICHD-3 diagnosis.
Secondary Headaches
o Headacheattributed to trauma or injury to the head and /or neck
o Headache attributed to cranial or cervical vascular disorder
o Headache attributed to non vascular intracranial disorder
o Headache attributed to a substance or its withdrawal
o Headache attributed to infection
o Headache attributed to disorder of homeostasis
o Headache or facial pain attributed to disorder of cranium, neck ,eyes etc.
o Headache attributed to psychiatric disorder
Ref: International Headache Society 2018
67.
Alcohol-induced Headache
• Headachecaused immediately, or after a delay, by ingestion of
alcohol (usually in the form of alcoholic beverages). It resolves
spontaneously.
• Immediate alcohol-induced Headache
• Delayed alcohol-induced Headache
Ref: International Headache Society 2018
68.
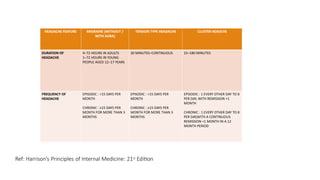
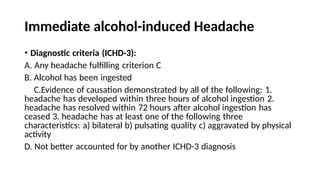
Immediate alcohol-induced Headache
•Diagnostic criteria (ICHD-3):
A. Any headache fulfilling criterion C
B. Alcohol has been ingested
C.Evidence of causation demonstrated by all of the following: 1.
headache has developed within three hours of alcohol ingestion 2.
headache has resolved within 72 hours after alcohol ingestion has
ceased 3. headache has at least one of the following three
characteristics: a) bilateral b) pulsating quality c) aggravated by physical
activity
D. Not better accounted for by another ICHD-3 diagnosis
69.
Delayed alcohol-induced Headache
•Diagnostic criteria (ICHD-3):
A. Any headache fulfilling criterion C
B. Alcohol has been ingested
C.Evidence of causation demonstrated by all of the following: 1.
headache has developed within 5–12 hours after ingestion of alcohol 2.
headache has resolved within 72 hours of onset 3. headache has at
least one of the following three characteristics: a) bilateral b) pulsating
quality c) aggravated by physical activity
D. Not better accounted for by another ICHD-3 diagnosis
70.
Opioid-overuse headache
• Diagnosticcriteria (ICHD-3):
A. Headache fulfilling criteria for Medication overuse headache
B.Regular intake of one or more opioids1 on 10 days/month for
>3 months
71.
Management of Opioid-overuseHeadache
• Hospitalization.
• Opioid withdrawn completely on the first day.
• Antiemetics and fluids administered as required.
• Clonidine for opioid withdrawal symptoms.
• For acute intolerable pain, Aspirin 1 g IV.
• IM Chlorpromazine can be helpful at night.
• 3-5 days into admission, a course of IV dihydrorgotamine (DHE),
administered every 8 hourly for 5 days.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
72.
Headache attributed topsychiatric disorder
• When a new headache occurs for the first time in close temporal relation
to a psychiatric disorder, and causation is confirmed, the headache is coded
as a secondary headache attributed to that disorder.
• When a pre-existing headache with the characteristics of a primary
headache disorder is made significantly worse (usually meaning a twofold
or greater increase in frequency and/or severity) in close temporal relation
to a psychiatric disorder, and causation is confirmed, both the initial
headache diagnosis and a diagnosis of Headache attributed to psychiatric
disorder (or one of its types) should be given.
Ref: International Headache Society 2018
73.
• Headache disordersoccur coincidentally with a number of psychiatric
disorders, including:
III.
I. depressive disorders,
II. anxiety disorders (separation anxiety disorder, panic disorder, social
anxiety disorder and generalized anxiety disorder) and
trauma- and stress-related disorders (reactive attachment disorder,
acute stress disorder, post-traumatic stress disorder and adjustment
disorders).
Ref: International Headache Society 2018
74.
• Evidence suggeststhat a comorbid psychiatric disorder tends to
worsen the course of Migraine and of Tension-type headache,
increasing the frequency and severity of the headache and/or making
it less responsive to treatment.
• Therefore, identification and treatment of any comorbid psychiatric
condition is important for the proper management of these
headaches.
Ref: International Headache Society 2018
75.
• In childrenand adolescents, primary headache disorders (Migraine,
Frequent episodic tension type headache and, Chronic tension-type
headache) are often comorbid with psychiatric disorder.
• Sleep disorders, post-traumatic stress disorder (PTSD), social anxiety
disorder (school phobia), attention-deficit/hyperactivity disorder
(ADHD), conduct disorder, learning disorder, enuresis, and tic disorder
should be carefully looked for and treated when found, considering
their negative burden in the disability and prognosis of paediatric
headache.
Ref: International Headache Society 2018
76.
• It shouldbe noted that evidence supporting psychiatric causes of
headache remains scarce.
• In cases, when there is no evidence of a causal relationship, both a
headache diagnosis and a separate psychiatric diagnosis should
be made.
Ref: International Headache Society 2018
77.
Secondary Headache Evaluation
•Meningitis: Acute, severe headache with stiff neck and fever,
accentuation of pain with eye movement.
• Intracranial Hemorrhage: Acute, maximal in <5 min, severe headache
lasting >5 minwith stiff neck but without fever.
• Brain Tumour: Nondescript-an intermittent deep, dull aching of
moderate intensity, which may worsen with exertion or change in
position.
• Glaucoma: Headache associated with nausea and vomiting, often
starting with severe eye pain. Examination reveals red eye with
fixed, moderately dilated pupil.
78.
• Neurologic Examination
•CT or MRI study of brain
• Lumbar Puncture
• Cervical spine evaluation by passive movement of head and by
imaging
• Renal status by urine examination and BP monitoring
• Eyes by fundoscopy, intraocular pressure measurement and
refraction.
Ref: Harrison’s Principles of Internal Medicine: 21st Edition
79.
Red Flags associatedwith Headache
• Thunderclap headache---Subarachnoid haemorrhage
• Atypical aura---Transient ischaemic attack, stroke, epilepsy
• Head trauma---Subdural haematoma
• Progressive headache---Intracranial space-occupying lesion
• Headache aggravated by postures, Papilledema---Intracranial hypertension
• Headache brought on by sneezing, coughing or exercise---Intracranial space-occupying lesion
• Visual impairment, periorbital pain--- Glaucoma
• Fever, altered mental status--- Encephalitis, Meningitis
• Headache onset at >50 years of age---Suggests secondary headache; consider temporal arteritis
• Neck stiffness---Meningitis, subarachnoid haemorrhage
• Focal neurological symptoms---Suggests secondary headache
Ref: Anna K. Eigenbrodt et al, 2021
80.
History Taking
• ONSET
•Childhood /early adult life-
migraine or TTH.
• New onset vs present
earlier
but worsened
• if acute /severe
• first and worst
• Rule out sec causes
• Subarachnoid HH
• Cerebral venous thrombosis
• Hypertensive crisis
• Thunderclap headache
LOCATION AND RADIATION
•Forehead- frontal sinus
•Temporal –migraine, temporal
arteritis
•Fronto temporal-
supratentorial lesions
•Occipital-post
fossa/c.spondylosis
•Orbital-cluster
•Holocranial-tension type
headache
•HEADACHE WITH
NECK/SHOULDER /ARM PAIN-
Cervicogenic pain
FREQUENCY AND TIMINGS
•Monthly /weekly/daily
headache.
•Diurnal variation
•More at night –hypnic
headache, cluster,
SUNCT.
•On awakening-OSA , HTN,
raised ICT or migraine.
•Seasonal pattern
•Trigeminal neuralgia –secs
•Cluster headache-15 to
120mns
•Migraine-4 to 72 hrs
•Episodic tension headache-
30mns to 7 days
81.
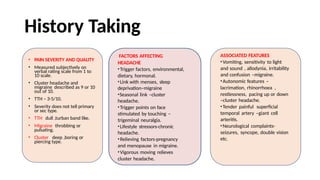
History Taking
• PAINSEVERITY AND QUALITY
• Measured subjectively on
verbal rating scale from 1 to
10 scale.
• Cluster headache and
migraine described as 9 or 10
out of 10.
• TTH – 3-5/10.
• Severity does not tell primary
or sec type.
• TTH- dull ,turban band like.
• Migraine- throbbing or
pulsating.
• Cluster –deep ,boring or
piercing type.
FACTORS AFFECTING
HEADACHE
•Trigger factors, environmental,
dietary, hormonal.
•Link with menses, sleep
deprivation–migraine
•Seasonal link –cluster
headache.
•Trigger points on face
stimulated by touching –
trigeminal neuralgia.
•Lifestyle stressors-chronic
headache.
•Relieving factors-pregnancy
and menopause in migraine.
•Vigorous moving relieves
cluster headache.
ASSOCIATED FEATURES
•Vomiting, sensitivity to light
and sound , allodynia, irritability
and confusion –migraine.
•Autonomic features –
lacrimation, rhinorrhoea ,
restlessness, pacing up or down
–cluster headache.
•Tender painful superficial
temporal artery –giant cell
arteritis.
•Neurological complaints-
seizures, syncope, double vision
etc.
82.
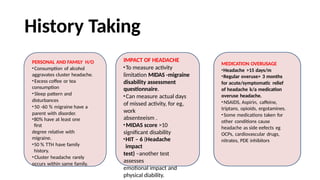
History Taking
PERSONAL ANDFAMILY H/O
•Consumption of alcohol
aggravates cluster headache.
•Excess coffee or tea
consumption
•Sleep pattern and
disturbances
•50 -60 % migraine have a
parent with disorder.
•80% have at least one
first
degree relative with
migraine.
•50 % TTH have family
history.
•Cluster headache rarely
occurs within same family.
IMPACT OF HEADACHE
•To measure activity
limitation MIDAS -migraine
disability assessment
questionnaire.
•Can measure actual days
of missed activity, for eg,
work
absenteeism .
•MIDAS score >10
significant disability
•HIT – 6 (Headache
impact
test) –another test
assesses
emotional impact and
physical diability.
MEDICATION OVERUSAGE
•Headache >15 days/m
•Regular overuse> 3 months
for acute/symptomatic relief
of headache k/a medication
overuse headache.
•NSAIDS, Aspirin, caffeine,
triptans, opioids, ergotamines.
•Some medications taken for
other conditions cause
headache as side eefects eg
OCPs, cardiovascular drugs,
nitrates, PDE inhibitors
83.
• During assessmentpay particular attention to explore the characteristics of
headache – site, onset, character of pain, associated symptoms, duration of
pain, frequency of headache, exacerbating and relieving factors and
severity of headache and relation of headache to menstrual cycles.
• Consider investigations/referral if headache features are suggestive of any
other underlying condition.
84.
• After establishingthe diagnosis, explain the diagnosis and
reassure the patient that other pathology has been excluded.
• Provide the options for management, include non-pharmacological
management in addition to medications.
• Choose treatment options as per patient profile.
![References
• ICHD-3,TheInternationalClassificationof
HeadacheDisorders,3rdedition.
• NICEHeadacheGuidelines[cited2021].
• Harrison’sPrinciplesof InternalMedicine:21st Edition
• RavishankarK,ChakravartyA, ChowdhuryD, ShuklaR, SinghS.
Guidelinesonthediagnosis
andthecurrentmanagementof
headacheandrelateddisorders.Annalsof IndianAcademyof
Neurology.2011 Jul;14(Suppl1):S40.
• BeckerWJ, FindlayT, MogaC,Scott NA, HarstallC,T
aenzerP.
Guidelineforprimarycare managementof headacheinadults.
Canadianfamilyphysician.2015Aug1;61(8):670-9.
• NEnglJMed2020;383:1866-76.DOI:10.1056/NEJMra1915327
• Goadsby, P.J., Goldberg,J.
&Silberstein,S.D.Migraineinpregnancy.BMJ336,1502–1504](https://image.slidesharecdn.com/headache-12-260118130032-9600c1a1/85/Headache-and-its-various-clinical-different-types-85-320.jpg)
















































