1. INTRODUCTION:
Herbal medicines are the synthesis of therapeutic experiences of
generations of practicing physicians of indigenous systems of
medicine for over hundreds of years while nutraceuticals are
nutritionally or medicinally enhanced foods with health benefits
of recent origin and marketed in developed countries. In 1991,
WHO developed guidelines for the assessment of herbal
medicine.
The earliest recorded evidence of their use in Indian, Chinese,
Egyptian, Greek, Roman and Syrian texts dates back to about
5000 years.
The classical Indian texts include Rigveda, Atherveda,
Charak Samhita and Sushruta Samhita. The herbal
Medicines/traditional medicaments have, therefore, been derived
from rich traditions of ancient civilizations and scientific
heritage.
WHY??
Herbal medicines are being used by about 80% of the world
population primarily in the developing countries for primary
health care. They have stood the test of time for their safety,
efficacy, cultural acceptability and lesser side effects.
Ancient literature also mentions herbal medicines for age-related
diseases namely memory loss, osteoporosis, diabetic wounds,
immune and liver disorders, etc. for which no modern medicine
or only palliative therapy is available. These drugs are made
from renewable resources of raw materials by ecofriendly
processes and will bring economic prosperity to the masses
growing these raw materials.
2. WORLD MARKET
As per available records, the herbal medicine market in 1991 in
the countries of the European Union was about $ 6 billion (may
be over $ 20 billion now), with Germany accounting for $ 3
billion, France $ 1.6 billion and Italy $ 0.6 billion. Incidentally
in Germany and France, herbal extracts are sold as prescription
drugs and are covered by national health insurance. In 1996, the
US herbal medicine market was about $ 4 billion and with the
current growth rate may be more than double by the turn of
century. Thus a reasonable guesstimate for current herbal
medicine market worldwide may be around $ 30–60 billion. The
Indian herbal drug market is about $ one billion and the export
of herbal crude extracts is about $ 80 million.
Germany holds the lead and has published individual
monographs on therapeutic benefits of more than 300 herbs. In
developing countries, China has compiled/generated data on
over 800 medicinal plants and exports large amounts of herbal
drugs. India has prepared only a few monographs and its exports
are dismal.
3. Herbal medicine scenario in India
The turnover of herbal medicines in India as over-the-counter
products, ethical and classical formulations and home remedies
of Ayurveda, Unani and Siddha systems of medicine is about $ 1
billion with a meagre export of about $ 80 million. Psyllium
seeds and husk, castor oil and opium extract alone account for
60% of the exports. 80% of the exports to developed countries
are of crude drugs and not finished formulations leading to low
revenue for the country. Thus the export of herbal medicines
from India is negligible despite the fact that the country has a
rich traditional knowledge and heritage of herbal medicine.
India is one of the 12 mega biodiversity centres having over
45,000 plant species. Its diversity is unmatched due to the
presence of 16 different agro climatic zones, 10 vegetative zones
and 15 biotic provinces. The country has 15,000–18,000
flowering plants, 23,000 fungi, 2500 algae, 1600 lichens, 1800
bryophytes and 30 million micro-organisms. India also has
equivalent to 3/4 of its land exclusive economic zone in the
ocean harbouring a large variety of flora and fauna, many of
them with therapeutic properties. About 1500 plants with
medicinal uses are mentioned in ancient texts and around 800
plants have been used in traditional medicine. The major
traditional sector pharmas, namely Himalaya, Zandu,
Dabur, Hamdard, Maharishi, etc. and modern sector pharmas,
namely Ranbaxy, Lupin, Allembic, etc. are standardizing their
herbal formulations by chromatography techniques like
TLC/HPLC finger printing, etc. There are about 7000 firms in
the small-scale sector manufacturing traditional medicines with
or without standardization.
4. REVIEW OF LITERATURE:
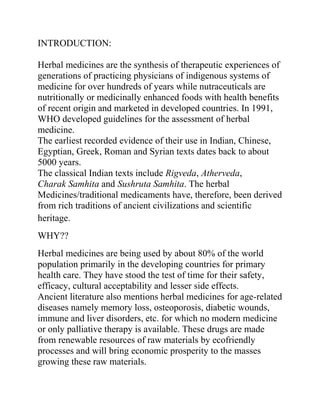
Macrothelypteris torresiana
Conservation status
Apparently Secure (NatureServe)
Scientific classification
Kingdom:
Plantae
Division:
Polypodiophyta
Class:
Polypodiopsida
Order:
Blechnales
Family:
Thelypteridaceae
Genus:
Macrothelypteris
Species:
M. torresiana
Binomial name
Macrothelypteris torresiana
(Gaudich.)
Synonyms
Thelypteris torresiana
5. Macrothelypteris torresiana is a species of fern which is native to tropical and subtropical
Africa and Asia. It has been introduced into other areas, including large parts of North and
South America.[1][2]
The species is assigned to different genera depending on how the family Thelypteridaceae
is classified. If the entire family is classified in Thelypteris, it is Thelypteris torresiana.
However, molecular data shows an affinity between a group of species which are
sometimes classified in Macrothelypteris,Phegopteris, and allied genera,[3] so it is common
to remove this species from Thelypteris and classify it as Macrothelypteris torresiana.
M. torresiana contains flavanoids which have been investigated for possible medicinal value
Description
Macrothelypteris torresiana is a robust fern with
a short creeping rhizome. Fronds are
three-pinnate, deeply divided, to 1.2 m long, with
a stalk 0.5 m. Sori are circular but not terminal
on the veins.
Fertile: September.
AFRICA
Southern Africa: South Africa - KwaZulu-Natal
Western Indian Ocean: Madagascar
ASIA-TEMPERATE
Eastern Asia: Japan - Honshu, Kyushu [s. & w.], Ryukyu Islands,
Shikoku [s.]; Taiwan
ASIA-TROPICAL
Indo-China: Indochina; Thailand
Malesia: Indonesia; Malaysia
6.
AUSTRALASIA
Australia: Australia - Queensland [e.]
New Zealand: New Zealand
PACIFIC
North-Central Pacific: United States - Hawaii
South-Central Pacific: French Polynesia
Southwestern Pacific: Samoa
it grows in open
places usually near water
FINDINGS TILL NOW:
Two new flavone derivatives (1 and 2) were isolated from the aerial parts of Macrothelypteris
torresiana, along with four known flavonoids: protoapigenin, apigenin, kaempferol and quercetin. The
structures were determined on the basis of spectroscopic data. Compound 1 showed weak cytotoxic
activity against human tumour cell lines HepG2, MCF7 and K562.
7. Preliminary Phytochemical Screening
MATERIALS AND METHODS
Collection of Plant Materials
Aerial parts of Macrothelypteris torresiana (Gaudich.) Ching
was obtained from a domestic stand in Kadiri, Anantapur
District, Andhra Pradesh State, India. The plant materials were
transported in polythene bags to the Research Laboratory of
Pharmacy, GITAM UNIVERSITY, VSKP, AP, INDIA. where
the study was carried out.
Processing of Plant Materials
The aerial parts were washed in running water and cut into small
bits to facilitate drying. The pieces of plant material were dried
in room temperature for 48 hours.The dried plant materials
(aerial parts) was taken separately and ground using an electric
blender to obtain a fine powder. The powder was further passed
through a 2mm sieve to obtain finer particles. The powdered
samples were stored in a clean glassware container until needed
for analysis.
8. Solvent Extraction Procedures
5g portions of powdered plant materials were each separately
dispersed in 50ml of each water, 70% ethanol, acetone,
methanol and hexane. The solution was left to stand at room
temperature for 24hrs and was filtered with Whatman No. 1
filter paper. The filtrate was used for the phytochemical
screening using the following tests.
Methods of Extraction of Medicinal Plants
Maceration
In this process, the whole or coarsely powdered crude drug is
placed in a stoppered container with the solvent and allowed to
stand at room temperature for a period of at least 3 days with
frequent agitation until the soluble matter has dissolved. The
mixture then is strained, the marc (the damp solid material) is
pressed, and the combined liquids are clarified by filtration or
decantation after standing.
circulatory extraction.
9. Infusion
Fresh infusions are prepared by macerating the crude drug for a
short period of time with cold or boiling water. These are dilute
solutions of the readily soluble constituents of crude drugs.
Digestion
This is a form of maceration in which gentle heat is used during
the process of extraction. It is used when moderately elevated
temperature is not objectionable. The solvent efficiency of
the menstrum is thereby increased.
Decoction
In this process, the crude drug is boiled in a specified volume of
water for a defined time; it is then cooled and strained or
filtered. This procedure is suitable for extracting water-soluble,
heatstable constituents. This process is typically used in
preparation of Ayurvedic extracts called “quath” or “kawath”.
The starting ratio of crude drug to water is fixed, e.g. 1:4 or
1:16; the volume is then brought down to one-fourth its original
volume by boiling during the extraction procedure. Then, the
concentrated extract is filtered and used as such or processed
further.
10. Percolation
This is the procedure used most frequently to extract active
ingredients in the preparation of tinctures and fluid extracts. A
percolator (a narrow, cone-shaped vessel open at both ends) is
generally used. The solid ingredients are moistened with an
appropriate amount of the specified menstruum and allowed to
stand for approximately 4 h in a well closed container, after
which the mass is packed and the top of the percolator is closed.
Additional menstruum is added to form a shallow layer above
the mass, and the mixture is allowed to macerate in the closed
percolator for 24 h. The outlet of the percolator then is opened
and the liquid contained therein is allowed to drip slowly.
Additional menstruum is added as required, until the percolate
measures about three-quarters of the required volume of the
finished product. The marc is then pressed and the expressed
liquid is added to the percolate. Sufficient menstruum is added
to produce the required volume, and the mixed liquid is clarified
by filtration or by standing followed by decanting.
11. Hot Continuous Extraction (Soxhlet)
In this method, the finely ground crude drug is placed in a
porous bag or “thimble” made of strong filter paper, which is
placed in chamber E of the Soxhlet apparatus (Figure 2). The
extracting solvent in flask A is heated, and its vapors condense
in condenser D. The condensed extractant drips into the thimble
containing the crude drug, and extracts it by contact. When the
12. level of liquid in chamber E rises to the top of siphon tube C, the
liquid contents of chamber E siphon into fl ask A. This process
is continuous and is carried out until a drop of solvent from the
siphon tube does not leave residue when evaporated. The
advantage of this method, compared to previously described
methods, is that large amounts of drug can be extracted with a
much smaller quantity of solvent. This effects tremendous
economy in terms of time, energy and consequently financial
inputs. At small scale, it is employed as a batch process only,
but it becomes much more economical and viable when
converted into a continuous extraction procedure on medium or
large scale.
13. Aqueous Alcoholic Extraction by Fermentation
Some medicinal preparations of Ayurveda (like asava and
arista) adopt the technique of fermentation for extracting the
active principles. The extraction procedure involves soaking the
crude drug, in the form of either a powder or a decoction
(kasaya), for a specified period of time, during which it
undergoes fermentation and generates alcohol in situ; this
facilitates the extraction of the active constituents contained in
the plant material. The alcohol thus generated also serves as a
preservative. If the fermentation is to be carried out in an earthen
vessel, it should not be new: water should first be boiled in the
vessel. In large-scale manufacture, wooden vats, porcelain jars
or metal vessels are used in place of earthen vessels. Some
examples of such preparations are karpurasava, kanakasava,
dasmularista. In Ayurveda, this method is not yet standardized
but, with the extraordinarily high degree of advancement in
fermentation technology, it should not be difficult to standardize
this technique of extraction for the production of herbal drug
extracts.
Counter-current Extraction
In counter-current extraction (CCE), wet raw material is
pulverized using toothed disc disintegrators to produce a fine
slurry. In this process, the material to be extracted is moved in
one direction (generally in the form of a fine slurry) within a
cylindrical extractor where it comes in contact with extraction
solvent. The further the starting material moves, the more
concentrated the extract becomes. Complete extraction is thus
possible when the quantities of solvent and material and their
flow rates are optimized. The process is highly efficient,
14. requiring little time and posing no risk from high temperature.
Finally, sufficiently concentrated extract comes out at one end of
the extractor while the marc (practically free of visible solvent)
falls out from the other end.
This extraction process has significant advantages:
A unit quantity of the plant material can be extracted with
much smaller volume of solvent as compared to other
methods like maceration, decoction, percolation.
CCE is commonly done at room temperature, which spares
the thermolabile constituents fromexposure to heat which is
employed in most other techniques.
As the pulverization of the drug is done under wet
conditions, the heat generated during comminution is
neutralized by water. This again spares the thermolabile
constituents from exposure to heat.
The extraction procedure has been rated to be more
efficient and effective than continuous hot extraction.
Ultrasound Extraction (Sonication)
The procedure involves the use of ultrasound with frequencies
ranging from 20 kHz to 2000 kHz; this increases the
permeability of cell walls and produces cavitation. Although the
process is useful in some cases, like extraction of rauwolfia root,
its large-scale application is limited due to the higher costs. One
disadvantage of the procedure is the occasional but known
deleterious effect of ultrasound energy (more than 20 kHz) on
the active constituents of medicinal plants through formation of
free radicals and consequently undesirable changes in the
15. drug molecules.
Supercritical Fluid Extraction
Supercritical fluid extraction (SFE) is an alternative sample
preparation method with general goals of reduced use of organic
solvents and increased sample throughput. The factors to
consider include temperature, pressure, sample volume, analyte
collection, modifier (cosolvent) addition, flow and pressure
control, and restrictors. Generally, cylindrical extraction vessels
are used for SFE and their performance is good beyond any
doubt. The collection of the extracted analyte following SFE is
another important step:
Significant analyte loss can occur during this step, leading the
analyst to believe that the actual efficiency was poor.
There are many advantages to the use of CO2 as the extracting
fluid. In addition to its favorable physical properties, carbon
dioxide is inexpensive, safe and abundant. But while carbon
dioxide is the preferred fluid for SFE, it possesses several
polarity limitations. Solvent polarity is important when
extracting polar solutes and when strong analyte-matrix
interactions are present. Organic solvents are frequently added
to the carbon dioxide extracting fluid to alleviate the polarity
16. limitations. Of late, instead of carbon dioxide, argon is being
used because it is inexpensive and more inert. The component
recovery rates generally increase with increasing pressure or
temperature: the highest recovery rates in case of argon are
obtained at 500 atm and 150° C.
The extraction procedure possesses distinct advantages:
The extraction of constituents at low temperature, which
strictly avoids damage from heat and some organic
solvents.
No solvent residues.
Environmentally friendly extraction procedure.
Phytochemical Screening
Test for Alkaloids (Wagner’s reagent)
A fraction of extract was treated with 3-5drops of Wagner’s
reagent [1.27g of iodine and 2g of potassium iodide in
17. 100ml of water] and observed for the formation of reddish
brown precipitate (or colouration).
Test for Carbohydrates (Molisch’s test)
Few drops of Molisch’s reagent were added to 2ml portion of
the various extracts. This was followed by addition of
2ml of conc. H2SO4 down the side of the test tube. The mixture
was then allowed to stand for two-three minutes.
Formation of a red or dull violet colour at the interphase of the
two layers was a positive test.
Test for Cardiac glycosides (Keller Kelliani’s test)
5ml of each extract was treated with 2ml of glacial acetic acid in
a test tube and a drop of ferric chloride solution was added to it.
This was carefully underlayed with 1ml concentrated sulphuric
acid. A brown ring at the interface indicated the presence of
deoxysugar characteristic of cardenolides. A violet ring may
appear below the ring while in the acetic acid layer, a greenish
ring may form.
18. Test for Flavonoids (Alkaline reagent test)
2ml of extracts was treated with few drops of 20% sodium
hydroxide solution. Formation of intense yellow colour, which
becomes colourless on addition of dilute hydrochloric acid,
indicates the presence of flavonoids.
IN VIVO METHODS FOR TESTING CENTRAL ANALGESIC ACTIVITY
HAFFNER’s tail clip method
Radiant heat method
Hot plate method .
Tail immersion test
Electrical stimulation of the tail
Grid shock test Tooth pulp stimulation
Monkey shock titration test
Formalin test in rats
ANTI PYRETIC ACTIVITY
Anti-pyretic testing in rats
Anti-pyretic testing in rabbits
IN VIVO METHODS FOR ANTI-INFLAMMATORY ACTIVITY
METHODS FOR TESTING ACUTE AND SUBACUTE INFLAMMATION
Ultraviolet erythema in guinea pigs
Vascular permeability
Inhibition of leukocyte adhesion to rat mesenteric venules in vivo
Oxazolone-induced ear edema in mice
Croton-oil ear edema in rats and mice
Paw edema
Pleurisy test
Granuloma pouch technique
Urate-induced synovitis
Methods for testing the proliferative phase (granuloma formation)
Cotton wool granuloma
Sponge implantation technique
Glass rod granuloma
Side effects of anti-inflammatory compounds